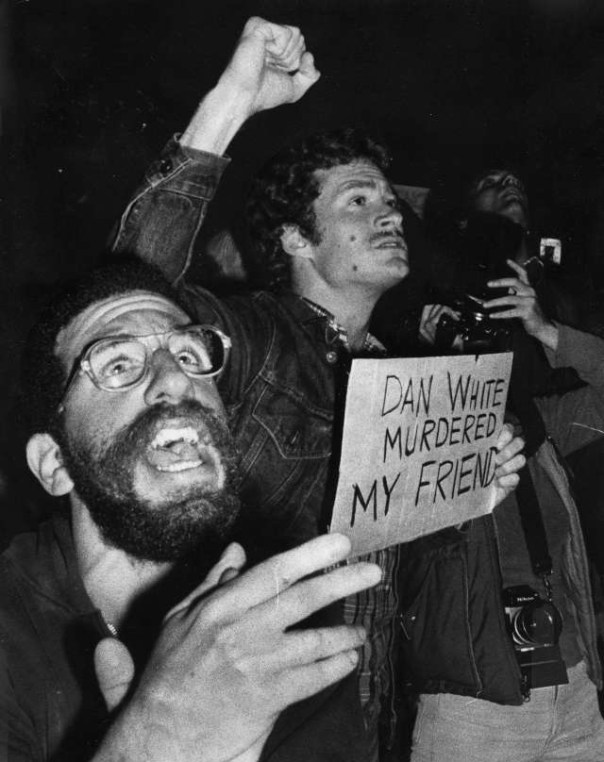
‘Dan White murdered my friend’: When anger boiled over into violence at City Hall and San Francisco police raided a Castro bar
On May 21, 1979, thousands of members of San Francisco’s predominantly gay Castro District community took to the streets to protest the lenient sentence received by Dan White for the murders of local politician and gay rights activist Harvey Milk and Mayor George Moscone. Their anger–combined with the actions of police who arrived to quell the scene–soon boiled over into rioting. The resulting violence affected San Francisco’s LGBT community for decades to come.
Harvey Milk rose to prominence as a gay rights activist and became the first openly gay person elected to a public office in the state of California when he was elected to the San Francisco Board of Supervisors in 1977. His murder, as well as that of Mayor Moscone, devastated not just the gay community, but the city as a whole.
Dan White was a former member of the Board of Supervisors who had clashed with Milk during their time serving the city together. In November of 1978, White resigned from his post, but changed his mind and asked to be reinstated. Mayor Moscone denied the request–with Milk lobbying against White’s reappointment. On November 27, White entered City Hall through a basement window and shot both men to death in their offices.
Six months later, White was convicted, not of first-degree murder, but voluntary manslaughter. White’s defense team had pointed to his diminished mental capacity and emotional state at the time of the murders, as indicated by the once-health conscious White consuming too much junk food– a ploy that became known as the “Twinkie Defense.” The jury-predominantly white, Roman Catholic and heterosexual—bought into it, recommending the lesser charge, which led to a sentence of just 7 years and 8 months.
When news of the verdict broke on the night of May 21, Cleve Jones–a close friend of Milk’s who would eventually go on to become one of the creators of the AIDS Quilt–spoke to a crowd of about 500 gatherers on Castro Street, and a peaceful march was quickly organized. By the time the crowd of protestors had made its second trip around the block, they were 1,500 strong. They then marched to City Hall, where their numbers expanded to an estimated 5,000.
As the crowd grew, so did the anger. Police soon arrived to try to control the situation, but that only served to enrage the crowd more. The police had raised over $100,000 for White’s defense–he was a former police officer–and many in the community believed the department had conspired to reduce White’s charges and sentencing. Although ordered to simply hold the crowd back, many officers began attacking the protestors with night sticks. Many had even taped over their badges, so as not to be identified.
Chaos erupted, as the crowd fought with police and destroyed a dozen police vehicles, as well as parts of City Hall itself. After three hours, officers moved in to quell the rioting for good, using tear gas in the process, and the crowd dispersed. In all, 59 officers and 124 protestors were injured, with about two dozen arrests made.
Hours later, several police officers gathered on their own to raid the Castro neighborhood, vandalizing a local bar and assaulting patrons. They shouted anti-gay slurs at the victims, and eventually turned their attention to attacking anyone that happened to be out on Castro Street.
After two hours, Police Chief Charles Gain was made aware of the rogue officers’ activities, and he made his way to the Castro to put a stop to it. No officers were reprimanded for the attacks, as officials were never able to determine who had ordered it, but the violence was finally over.
The next day, on what would have been Milk’s 49th birthday, 20,000 San Franciscans gathered to remember him. That October, more than 75,000 people marched for gay rights in Washington, D.C., and gay rights activists from around the country were inspired to continue their fight.
In San Francisco, the riots led to a wave of political changes, as more and more LGBT politicians were elected over the next decades. LGBT presence on the police forced also dramatically increased, and has continued to increase to this day.
There are still those out there who think AZT saved lives…it didn’t!I took it!I know!Will & Deni McIntyre—Getty Images
Today, if someone is diagnosed with HIV, he or she can choose among 41 drugs that can treat the disease. And there’s a good chance that with the right combination, given at the right time, the drugs can keep HIV levels so low that the person never gets sick.
That wasn’t always the case. It took seven years after HIV was first discovered before the first drug to fight it was approved by the U.S. Food and Drug Administration (FDA). In those first anxious years of the epidemic, millions were infected. Only a few thousand had died at that point, but public health officials were racing to keep that death rate from spiking — the inevitable result if people who tested positive weren’t treated with something.
As it turned out, their first weapon against HIV wasn’t a new compound scientists had to develop from scratch — it was one that was already on the shelf, albeit abandoned. AZT, or azidothymidine, was originally developed in the 1960s by a U.S. researcher as way to thwart cancer; the compound was supposed to insert itself into the DNA of a cancer cell and mess with its ability to replicate and produce more tumor cells. But it didn’t work when it was tested in mice and was put aside.
Two decades later, after AIDS emerged as new infectious disease, the pharmaceutical company Burroughs Wellcome, already known for its antiviral drugs, began a massive test of potential anti-HIV agents, hoping to find anything that might work against this new viral foe. Among the things tested was something called Compound S, a re-made version of the original AZT. When it was throw into a dish with animal cells infected with HIV, it seemed to block the virus’ activity.
The company sent samples to the FDA and the National Cancer Institute, where Dr. Samuel Broder, who headed the agency, realized the significance of the discovery. But simply having a compound that could work against HIV wasn’t enough. In order to make it available to the estimated millions who were infected, researchers had to be sure that it was safe and that it would indeed stop HIV in some way, even if it didn’t cure people of their infection. At the time, such tests, overseen by the FDA, took eight to 10 years.
Patients couldn’t wait that long. Under enormous public pressure, the FDA’s review of AZT was fast tracked — some say at the expense of patients.
Scientists quickly injected AZT into patients. The first goal was to see whether it was safe — and, though it did cause side effects (including severe intestinal problems, damage to the immune system, nausea, vomiting and headaches) it was deemed relatively safe. But they also had to test the compound’s effectiveness. In order to do so, a controversial trial was launched with nearly 300 people who had been diagnosed with AIDS. The plan was to randomly assign the participants to take capsules of the agent or a sugar pill for six months. Neither the doctor nor the patient would know whether they were on the drug or not.
After 16 weeks, Burroughs Wellcome announced that they were stopping the trial because there was strong evidence that the compound appeared to be working. One group had only one death. Even in that short period, the other group had 19. The company reasoned that it wouldn’t be ethical to continue the trial and deprive one group of a potentially life-saving treatment.
Those results — and AZT — were heralded as a “breakthrough” and “the light at the end of the tunnel” by the company, and pushed the FDA approve the first AIDS medication on March 19, 1987, in a record 20 months.
But the study remains controversial. Reports surfaced soon after that the results may have been skewed since doctors weren’t provided with a standard way of treating the other problems associated with AIDS — pneumonia, diarrhea and other symptoms — which makes determining whether the AZT alone was responsible for the dramatic results nearly impossible. For example, some patients received blood transfusions to help their immune systems; introducing new, healthy blood and immune cells could have helped these patients battle the virus better. There were also stories of patients from the 12 centers where the study was conducted pooling their pills, to better the chances that they would get at least some of the drug rather than just placebos.
And there were still plenty of questions left unanswered about the drug when it was approved. How long did the apparent benefits last? Could people who weren’t sick yet still benefit? Did they benefit more than those further along in their disease?
Such uncertainty would not be acceptable with a traditional approval, but the urgent need to have something in hand to fight the growing epidemic forced FDA’s hand. The people in the trial were already pressuring the company and the FDA to simply release the drug — if there were something that worked against HIV, they said, then it was not ethical to withhold it.
The drug’s approval remains controversial to this day, but in a world where treatment options are so far advanced it can be hard to imagine the sense of urgency and the social pressure permeating the medical community at the time. AIDS was an impending wave that was about to crash on the shores of an unsuspecting — and woefully unprepared — populace. Having at least one drug that worked, in however limited a way, was seen as progress.
But even after AZT’s approval, activists and public health officials raised concerns about the price of the drug. At about $8,000 a year (more than $17,000 in today’s dollars) — it was prohibitive to many uninsured patients and AIDS advocates accused Burroughs Wellcome of exploiting an already vulnerable patient population.
In the years since, it’s become clear that no single drug is the answer to fighting HIV. People taking AZT soon began showing rising virus levels — but the virus was no longer the same, having mutated to resist the drug. More drugs were needed, and AIDS advocates criticized the FDA for not moving quickly enough to approve additional medications. And side effects including heart problems, weight issues and more reminded people that anything designed to battle a virus like HIV was toxic.
Today, there are several classes of HIV drugs, each designed to block the virus at specific points in its life cycle. Used in combination, they have the best chance of keeping HIV at bay, lowering the virus’s ability to reproduce and infect, and ultimately, to cause death. These so-called antiretroviral drugs have made it possible for people diagnosed with HIV to live long and relatively healthy lives, as long they continue to take the medications.
And for most of these people, their therapy often still includes AZT.
AIDS HOPES DASHED BY TERRIBLE TRUTH ON AZT
It was the drug that held out hope to people carrying the world’s most feared virus. It had the power to move share prices by millions. What it could not do was help people facing AIDS.
This weekend the truth about AZT is in the open: a comprehensive trial, so big it equals all the other research put together, shows that the drug which dominates AIDS treatment has no effect in delaying the onset of the disease. After all the promise and the profits, AZT has nothing to offer people with HIV.
The findings came in the final report on the Anglo-French Concorde trial, published yesterday in The Lancet. Some 1,749 patients with HIV, but who showed no symptoms, were given either the drug or a placebo. There was no statistical difference in the progress of the two groups: after three years 18% had AIDS or were dead.
The results leave a terrible void for the 12m people worldwide said to be infected with the virus, and crush any remaining hopes that AZT might delay the onset of symptoms. They also raise questions as to how those hopes were fuelled in the first place.
Doubts about AZT were first revealed by The Sunday Times five years ago. A painstaking investigation showed that AZT had been rushed to market on the back of a flawed study that was supposed to demonstrate its effectiveness.
The American Food and Drug Administration (FDA), responsible for protecting the public from risk, had been aware of flaws in the trial, but gave AZT approval. Documents obtained under the American Freedom of Information Act showed that records compiled during the trial had been altered, giving the drug a more favourable record; “multiple deviations” from the terms of the study had occurred; and FDA investigators had argued for data from one centre to be dropped entirely from the results. A senior FDA official believed AZT should not be granted a licence, but was overruled.
The doubts did nothing to inhibit Wellcome, AZT’s maker, from promoting its drug. Patients with HIV, but without AIDS symptoms, were the new target. They are worth more money because there are more of them and because they have longer to live.
To show the drug’s usefulness to this lucrative group, Wellcome trumpeted a big American trial called Protocol 019. The trial was halted in August 1989, after less than two years, on the grounds that it had already shown such benefit to HIV-positive people it would be unethical not to give the drug to all who wanted it.
Such “benefit” was judged only by time free from disease. A new analysis of the trial data, however, reaches a similar conclusion to Concorde: that AZT is essentially useless.
The original results were announced with a fanfare by the National Institute of Allergy and Infectious Diseases, which sponsored it with Wellcome’s support. In London, The Independent newspaper gave its front page to the findings, under the headline “AIDS drug offers lease of life”.
The very different picture painted by last month’s analysis, in the New England Journal of Medicine, comes after investigators paid more attention to the drug’s side-effects. These can include anaemia, liver damage, fatigue, nausea, headaches and sometimes a collapse in white blood cells, making patients more prone to disease.
The researchers looked at the average time patients experienced neither a progression of disease nor an adverse effect. Those treated with low doses of AZT were found to suffer a reduction in quality of life “due to severe side-effects of therapy” that approximately equalled any benefit from slowing down the disease; people on higher doses suffered even greater side-effects, outweighing the supposed benefit.
Dr Peter Duesberg, the American virus expert who has claimed for years that AZT is not a rational therapy, says it is clear that the original claims were completely ill-founded. “The opposite interpretations of the same data lead me to conclude that those responsible are not acting as scientists; they are acting as politicians.
“When the time is ripe to say that AZT is detrimental, that it actually hurts, the interpretation will change again.”
For patients with AIDS-related symptoms, AZT will continue to be prescribed: the consensus remains that it gives a temporary benefit.
For those without symptoms, hope centres on combinations of drugs, or on other approaches such as gene therapy. However, Professor Ian Weller, of the Middlesex hospital in London, who was the principal British investigator in the Concorde trial, is alarmed by the drive to give AIDS patients an AZT drug cocktail as if it were already an established therapy.
“There’s a suspicion of more toxicity if you combine it with other treatment, and we are a long way from showing an important clinical benefit, or that it is safer than AZT on its own,” he said. “There are physicians who are jumping the gun.”
As late as Thursday, Wellcome was insisting that AZT “remains the best weapon we have to slow the progress of the disease”. Dr Trevor Jones, its research director, said: “The question is where in the course of the disease you begin.” *
AIDS and the AZT Scandal: SPIN’s 1989 Feature, ‘Sins of Omission’
The story of AZT, one of the most toxic, expensive, and controversial drugs in the history of medicine
At the end of 1989, two years after we had started the highly controversial AIDS column in SPIN, we published an article by Celia Farber called “Sins of Omission” about the truly bad and corrupt science surrounding promoting AZT as a treatment for the syndrome of diseases.
Celia was the editor and frequent writer of the column and unearthed hard evidence of the cold-bloodedness of the AIDS establishment pushing a drug that was worse than the disease, and killed faster than the natural progression of AIDS left untreated. AZT had been an abandoned cancer drug, discarded because of it’s fatal toxicity, resurrected in the cynical belief that AIDS patients were going to die anyway, so trying it out was sort of like playing with the house’s money. Because the drug didn’t require the usual massively expensive research and trial processes, having gone through that years earlier, it was insanely profitable for its maker, Burroughs Wellcome. It was a tragically perfect storm of windfall profits, something to pacify AIDS activists and the media, and a convenient boom to the patent holders for HIV testing.
Celia — who should get the Congressional Medal of Honor for her brave and relentless reporting, here and throughout the ten years we ran the column — exposed the worthlessness of the drug, the shady studies and deals to suppress the negative findings, and its awful and final consequences. This piece very literally changed the media’s view of AIDS and sharpened their discerning and skeptical eye. And soon after, AZT was once again shelved, hopefully this time forever.
Many times over the years since, people have come up to me and said that reading this article saved their lives, that they either stopped taking the drug and their health improved vastly, or they never took it because of what we reported. Nothing ever made me prouder.
— Bob Guccione Jr., founder of SPIN, October 3, 2015
[This story was originally published in the November 1989 issue of SPIN. In honor of SPIN’s 30th anniversary, we’ve republished this piece as part of our ongoing “30 Years, 30 Stories” series.]
On a cold January day in 1987, inside one of the brightly-lit meeting rooms of the monstrous FDA building, a panel of 11 top AIDS doctors pondered a very difficult decision. They had been asked by the FDA to consider giving lightning-quick approval to a highly toxic drug about which there was very little information. Clinically called Zidovudine, but nicknamed AZT after its components, the drug was said to have shown a dramatic effect on the survival of AIDS patients. The study that had brought the panel together had set the medical community abuzz. It was the first flicker of hope — people were dying much faster on the placebo than on the drug.
But there were tremendous concerns about the new drug. It had actually been developed a quarter of a century earlier as a cancer chemotherapy, but was shelved and forgotten because it was so toxic, very expensive to produce, and totally ineffective against cancer. Powerful, but unspecific, the drug was not selective in its cell destruction.
Drug companies around the world were sifting through hundreds of compounds in the race to find a cure, or at least a treatment, for AIDS. Burroughs Wellcome, a subsidiary of Wellcome, a British drug company, emerged as the winner. By chance, they sent the failed cancer drug, then known as Compound S, to the National Cancer Institute along with many others to see if it could slay the AIDS dragon, HIV. In the test tube at least, it did. At the meeting, there was a lot of uncertainty and discomfort with AZT. The doctors who had been consulted knew that the study was flawed and that the long-range effects were completely unknown. But the public was almost literally baying at the door. Understandably, there was immense pressure on the FDA to approve AZT, considering the climate of fear and anger all around.*
Everybody was worried about this one. To approve it, said Ellen Cooper, an FDA director, would represent a “significant and potentially dangerous departure from our normal toxicology requirements.” Just before approving the drug, one doctor on the panel, Calvin Kunin, summed up their dilemma. “On the one hand,” he said, “to deny a drug which decreases mortality in a population such as this would be inappropriate. On the other hand, to use this drug widely, for areas where efficacy has not been demonstrated, with a potentially toxic agent, might be disastrous.”
“We do not know what will happen a year from now,” said panel chairman Dr. Itzhak Brook. “The data is just too premature, and the statistics are not really well done. The drug could actually be detrimental.” A little later, he said he was also “struck by the fact that AZT does not stop deaths. Even those who were switched to AZT still kept dying.”
“I agree with you,” answered another panel member, “there are so many unknowns. Once a drug is approved, there is no telling how it could be abused. There’s no going back.” Burroughs Wellcome reassured the panel that they would provide detailed two-year follow-up data, and that they would not let the drug get out of its intended parameters: as a stopgap measure for very sick patients.
Dr. Brook was not won over by the promise. “If we approve it today, there will not be much data. There will be a promise of data,” he predicted, “but then the production of data will be hampered.” Brook’s vote was the only one cast against approval.
“There was not enough data, not enough follow-up,” Brook recalls. “Many of the questions we asked the company were answered by, ‘We have not analyzed the data yet,’ or, ‘We do not know.’ I felt that there was some promising data, but was very worried about the price being paid for it. The side effects were so very severe. It was chemotherapy. Patients were going to need blood transfusions, that’s very serious.”
“The committee was tending to agree with me,” says Brook, “that we should wait a little bit, be more cautious. But once the FDA realized we were intending to reject it, they applied political pressure. At about 4 p.m., the head of the FDA’s Center for Drugs and Biologics asked permission to speak, which is extremely unusual. Usually they leave us alone. But he said to us, ‘Look, if you approve the drug, we can assure you that we will work together with Burroughs Wellcome and make sure the drug is given to the right people.’ It was like saying ‘please do it.’”
Brad Stone, FDA press officer, was at that meeting. He says he doesn’t recall that particular speech, but that there is nothing “unusual” about FDA officials making such speeches at advisory meetings. “There was no political pressure,” he says. “The people in that meeting approved the drug because the data the company had produced proved it was prolonging life. Sure it was toxic, but they concluded that the benefits clearly outweighed the risks.” The meeting ended. AZT, which several members of the panel still felt uncomfortable with and feared could be a time bomb, was approved.
Flash forward: August 17, 1989. Newspapers across America banner-headlined that AZT had been “proven to be effective in HIV antibody-positive, asymptomatic, and early ARC patients,” even though one of the panel’s main concerns was that the drug should only be used in a last-case scenario for critically-ill AIDS patients, due to the drug’s extreme toxicity. Dr. Anthony Fauci, head of the National Institutes of Health (NIH), was now pushing to expand prescription.
The FDA’s traditional concern had been thrown to the wind. Already the drug had spread to 60 countries and an estimated 20,000 people. Not only had no new evidence allayed the initial concerns of the panel, but the follow-up data, as Dr. Brook predicted, had fallen by the wayside. The beneficial effects of the drug had proven to be temporary. The toxicity, however, stayed the same.
The majority of those in the AIDS-afflicted and medical communities held the drug up as the first breakthrough on AIDS. For better or worse, AZT had been approved faster than any drug in FDA history, and activists considered it a victory. The price paid for the victory, however, was that almost all government drug trials, from then on, focused on AZT — while over 100 other promising drugs were left uninvestigated.
Burroughs Wellcome stock went through the roof when the announcement was made. At a price of $8.000 per patient per year (not including blood-work and transfusions), AZT is the most expensive drug ever marketed. Burroughs Wellcome’s gross profits for next year are estimated at $230 million. Stock market analysts predict that Burroughs Wellcome may be selling as much as $2 billion worth of AZT, under the brand name Retrovir, each year by the mid-1990s — matching Burroughs Wellcome’s total sales for all its products last year.
“Does AZT do anything? Yes, it does. But the evidence that it does something against HIV is really not there.”
AZT is the only antiretroviral drug that has received FDA approval for treatment of AIDS since the epidemic began ten years ago, and the decision to approve it was based on a single study that has long been declared invalid. The study was intended to be a “double-blind placebo-controlled study,” the only kind of study that can effectively prove whether or not a drug works. In such a study, neither patient nor doctor is supposed to know if the patient is getting the drug or a placebo. In the case of AZT, the study became unblinded on all sides, after just a few weeks.
Both sides contributed to the unblinding. It became obvious to doctors who was getting what because AZT causes such severe side effects that AIDS per se does not. Furthermore, a routine blood count known as a CMV, which clearly shows who is on the drug and who is not, wasn’t whited out in the reports. Both of these facts were accepted and confirmed by both the FDA and Burroughs Wellcome, who conducted the study.
Many of the patients who were in the trial admitted that they had analyzed their capsules to find out whether they were getting the drug. If they weren’t, some bought the drug on the underground market. Also, the pills were supposed to be indistinguishable by taste, but they were not. Although this was corrected early on, the damage was already done. There were also reports that patients were pooling pills out of solidarity to each other. The study was so severely flawed that its conclusions must be considered, by the most basic scientific standards, unproven.
The most serious problem with the original study, however, is that it was never completed. Seventeen weeks into the study, when more patients had died in the placebo group, the study was stopped, five months prematurely, for “ethical” reasons: It was considered unethical to keep giving people a placebo when the drug might keep them alive longer. Because the study was stopped short, and all subjects were put on AZT, no scientific study can ever be conducted to prove unequivocally whether AZT does prolong life.
Dr. Brook, who voted against approval, warned at the time that AZT, being the only drug available for doctors to prescribe to AIDS patients, would probably have a runaway effect. Approving it prematurely, he said, would be like “letting the genie out of the bottle.”
Brook pointed out that since the drug is a form of chemotherapy, it should only be prescribed by doctors who have experience with chemotherapeutic drugs. Because of the most severe toxic effect of AZT — cell depletion of the bone marrow —patients would need frequent blood transfusions. As it happened, AZT was rampantly prescribed as soon as it was released, way beyond its purported parameters. The worst-case scenario had come true: Doctors interviewed by the New York Times later in 1987 revealed that they were already giving AZT to healthy people who had tested positive for antibodies to HIV.
The FDA’s function is to weigh a drug’s efficacy against its potential hazards. The equation is simple and obvious: A drug must unquestionably repair more than it damages, otherwise the drug itself may cause more harm than the disease it is supposed to fight. Exactly what many doctors and scientists fear is happening with AZT.
“I personally do not prescribe AZT. I have continued to experience that people live longer who are not on it.”
AZT was singled out among hundreds of compounds when Dr. Sam Broder, the head of the National Cancer Institute (NCI), found that it “inhibited HIV viral replication in vitro.” AIDS is considered a condition of immune suppression caused by the HIV virus replicating and eating its way into T-4 cells, which are essential to the immune system. HIV is a retrovirus which contains an enzyme called reverse transcriptase that converts viral RNA to DNA. AZT was thought to work by interrupting this DNA synthesis, thus stopping further replication of the virus.
While it was always known that the drug was exceedingly toxic, the first study concluded that “the risk/benefit ratio was in favor of the patient.”
In the study that won FDA approval for AZT, the one fact that swayed the panel of judges was that the AZT group outlived the placebo group by what appeared to be a landslide. The ace card of the study, the one that canceled out the issue of the drug’s enormous toxicity, was that 19 persons had died in the placebo group and only one in the AZT group. The AZT recipients were also showing a lower incidence of opportunistic infections.
While this data staggered the panel that approved the drug, other scientists insisted that it meant nothing — because it was so shabbily gathered, and because of the unblinding. Shortly after the study was stopped, the death rate accelerated in the AZT group. “There was no great difference after a while,” says Dr. Brook, “between the treated and the untreated group.”
“That study was so sloppily done that it really didn’t mean much,” says Dr. Joseph Sonnabend, a leading New York City AIDS doctor. Dr. Harvey Bialy, scientific editor of the journal Biotechnology, is stunned by the low quality of science surrounding AIDS research. When asked if he had seen any evidence of the claims made for AZT, that it “prolongs life” in AIDS patients, Bialy said, “No, I have not seen a published study that is rigorously done, analyzed, and objectively reported.”
Bialy, who is also a molecular biologist, is horrified by the widespread use of AZT, not just because it is toxic, but because, he insists, the claims its widespread use are based upon are false. “I can’t see how this drug could be doing anything other than making people very sick,” he says.
The scientific facts about AZT and AIDS are indeed astonishing. Most ironically, the drug has been found to accelerate the very process it was said to prevent: the loss of T-4 cells.
“Undeniably, AZT kills T-4 cells [white blood cells vital to the immune system],” says Bialy. “No one can argue with that. AZT is a chain-terminating nucleotide, which means that it stops DNA replication. It seeks out any cell that is engaged in DNA replication and kills it. The place where most of this replication is taking place is in the bone marrow. That’s why the most common and severe side effect of the drug is bone marrow toxicity. That is why they [patients] need blood transfusions.”
AZT has been aggressively and repeatedly marketed as a drug that prolongs survival in AIDS patients because it stops the HIV virus from replicating and spreading to healthy cells. But, says Bialy: “There is no good evidence that HIV actively replicates in a person with AIDS, and if there isn’t much HIV replication to stop, it’s mostly killing healthy cells.”
University of California at Berkeley scientist Dr. Peter Duesberg drew the same conclusion in a paper published in Proceedings, the journal of the National Academy of Sciences. Duesberg, whose paper addressed his contention that HIV is not a sufficient cause for AIDS, wrote: “Even if HIV were to cause AIDS, it would hardly be a legitimate target for AZT therapy, because in 70 to 100 percent of antibody-positive persons, proviral DNA is not detectable… and its biosynthesis has never been observed.”
As a chemotherapeutic drug, explained Duesberg, AZT “kills dividing blood cells and other cells,” and is thus “directly immunosuppressive.”
“The cell is almost a million-fold bigger target than the virus, so the cell will be much, much more sensitive,” says Duesberg. “Only very few cells, about one in 10,000, are actively making the virus containing DNA, so you must kill incredibly large numbers of cells to inhibit the virus. This kind of treatment could only theoretically help if you have a massive infection, which is not the case with AIDS. Meanwhile, they’re giving this drug that ends up killing millions of lymphocytes [white blood cells]. It’s beyond me how that could possibly be beneficial.”
“It doesn’t really kill them,” Burroughs Wellcome scientist Sandra Lehrman argues. “You don’t necessarily have to destroy the cell, you can just change the function of it. Furthermore, while the early data said that only very few cells were infected, new data says that there may be more cells infected. We have more sensitive detection techniques now.”
“Changes their function? From what — functioning to not functioning? Another example of mediocre science,” says Bialy. “The ‘sensitive detection technique’ to which Dr. Lehrman refers, PCR, is a notoriously unreliable one upon which to base quantitative conclusions.”
When specific questions about the alleged mechanisms of AZT are asked, the answers are long, contradictory, and riddled with unknowns. Every scientific point raised about the drug is eventually answered with the blanket response, “The drug is not perfect, but it’s all we have right now.” About the depletion of T-4 cells and other white cells, Lehrman says, “We don’t know why T-4 cells go up at first, and then go down. That is one of the drug mechanisms that we are trying to understand.”
When promoters of AZT are pressed on key scientific points, whether at the NIH, FDA, Burroughs Wellcome, or an AIDS organization, they often become angry. The idea that the drug is “doing something,” even though this is invariably followed with irritable admissions that there are “mechanisms about the drug and disease we don’t understand,” is desperately clung to. It is as if, in the eye of the AIDS storm, the official, government-agency sanctioned position is immunized against critique. Skepticism and challenge, so essential to scientific progress and so prevalent in every other area of scientific endeavor, is not welcome in the AZT debate, where it is arguably needed more than anywhere else.
The results, finally and ironically, are what damns AZT.
The toxic effects of AZT, particularly bone marrow suppression and anemia, are so severe that up to 50 percent of all AIDS and ARC patients cannot tolerate it and have to be taken off it. In the approval letter that Burroughs Wellcome sent to the FDA, all of 50 additional side effects of AZT, aside from the most common ones, were listed. These included: loss of mental acuity, muscle spasms, rectal bleeding, and tremors.
Anemia, one of AZT’s common side effects, is the depletion of red blood cells, and, according to Duesberg, “Red blood cells are the one thing you cannot do without. Without red cells, you cannot pick up ???gen.”
Fred, a person with AIDS, was put on AZT and suffered such severe anemia from the drug he had to be taken off it. In an interview in the AIDS handbook Surviving and Thriving With AIDS, he described what anemia feels like to editor Michael Callen: “I live in a studio and my bathroom is a mere five-step walk from my bed. I would just lie there for two hours; I couldn’t get up to take those five steps. When I was taken to the hospital, I had to have someone come over to dress me. It’s that kind of severe fatigue. The quality of my life was pitiful… I’ve never felt so bad… I stopped the AZT and the mental confusion, the headaches, the pains in the neck, the nausea, all disappeared within a 24-hour period.”
“I feel very good at this point,” Fred went on. “I feel like the quality of my life was a disaster two weeks ago. And it really was causing a great amount of fear in me, to the point where I was taking sleeping pills to calm down. I was so worried. I would totally lose track of what I was saying in the middle of a sentence. I would lose my directions on the street.”
“Many AIDS patients are anemic even before they receive the drug,” says Burroughs Wellcome’s Dr. Lehrman, “because HIV itself can infect the bone marrow and cause anemia.”
This argument betrays a bizarre reasoning. If AIDS patients are already burdened with problems such as immune suppression, bone marrow toxicity, and anemia, is compounding these problems an improvement?
“Yes, AZT is a form of chemotherapy,” says the man who invented the compound a quarter-century ago, Jerome Horwitz. “It is cytotoxic, and as such, it causes bone marrow toxicity and anemia. There are problems with the drug. It’s not perfect. But I don’t think anybody would agree that AZT is of no use. People can holler from now until doomsday that it is toxic, but you have to go with the results.”
The results, finally and ironically, are what damns AZT. Several studies on the clinical effects of AZT — including the one that Burroughs Wellcome’s approval was based on — have drawn the same conclusion: that AZT is effective for a few months, but that its effect drops off sharply after that. Even the original AZT study showed that T-4 cells went up for a while and then plummeted. HIV levels went down, and then came back up. This fact was well-known when the advisory panel voted for approval. As panel member Dr. Stanley Lemon said in the meeting, “I am left with the nagging thought that after seeing several of these slides, that after 16 to 24 weeks — 12 to 16 weeks, I guess — the effect seems to be declining.”
A follow-up meeting, two weeks after the original Burroughs Wellcome study, was scheduled to discuss the long-range effects of AZT and the survival statistics. As one doctor present at that meeting in May 1988 recalls, “They hadn’t followed up the study. Anything that looked beneficial was gone within half a year. All they had were some survival statistics averaging 44 weeks. The p24 didn’t pan out and there no persistent improvement in T-4 cells.”
HIV levels in the blood are measured by an antigen called p24. Burroughs Wellcome made the claim that AZT lowered this level, that is, lowered the amount of HIV in the blood. At the first FDA meeting, Burroughs-Welcome emphasized how the drug had “lowered” the p24 levels; at the follow-up meeting they didn’t even mention it.
As that meeting was winding down, Dr. Michael Lange, head of the AIDS program at St. Luke’s-Roosevelt Hospital in New York spoke up about this. “The claim of AZT is made on the fact that it is supposed to have an antiviral effect,” he said to Burroughs Wellcome, “and on this we have seen no data at all… Since there is a report in the Lancet [a leading British medical journal] that after 20 weeks or so, in many patients p24 came back, do you have any data on that?”
They didn’t.
“What counts is the bottom line,” one of the scientists representing Burroughs Wellcome summed up, “the survival, the neurologic function, the absence of progression and the quality of life, all of which are better. Whether you call it better because of some antiviral effect, or some other antibacterial effect, they are still better.”
Dr. Lange suggested that the drug may be effective in the same way a simple anti-inflammatory, such as aspirin, is effective. An inexpensive, nontoxic drug called Indomecithin, he pointed out, might serve the same function, without the devastating side effects.
One leading AIDS researcher, who was part of the FDA approval process, says today: “Does AZT do anything? Yes, it does. But the evidence that it does something against HIV is really not there.”
“There have always been drugs that we use without knowing exactly how they work,” says Nobel Prize winner Walter Gilbert. “The really important thing to look at is the clinical effect. Is the drug helping or isn’t it?”
A physician with extensive experience with AIDS patients who asked to remain anonymous told SPIN, point blank: “I personally do not prescribe AZT. I have continued to experience that people live longer who are not on it.”
“I’m living proof that AZT works,” says one person with ARC on AZT. “I’ve been on it for two years now, and I’m certainly healthier than I was two years ago. It’s not a cure-all, it’s not a perfect drug, but it’s effective. It’s slowing down the progression of the disease.”
“Sometimes I fee like I’m swallowing Drano,” says another. “I mean, sometimes I have problems swallowing. I just don’t like the idea of taking something that foreign to my body. But every six hours, I’ve got to swallow it. Until something better comes along, this is what is available to me.”
“I am absolutely convinced that people enjoy a better quality of life and survive longer who do not take AZT,” says Gene Fedorko, President of Health Education AIDS Liaison (HEAL). “I think it’s horrible the way people are bullied by their doctors to take this drug. We get people coming to us shaking and crying because their doctors said they’ll die if they don’t take AZT. That is an absolute lie.” Fedorko has drawn his conclusion from years of listening to the stories of people struggling to survive AIDS at HEAL’s weekly support group.
“I wouldn’t take AZT if you paid me,” says Michael Callen, cofounder of New York City’s PWA coalition, Community Research Initiative, and editor of several AIDS journals. Callen has survived AIDS for over seven years without the help of AZT. “I’ve gotten the s–t kicked out of me for saying this, but I think using AZT is like aiming a thermonuclear warhead at a mosquito. The overwhelming majority of long-term survivors I’ve known have chosen not to take AZT.”
“I’m convinced that if you gave AZT to a perfectly healthy athlete he would be dead in five years.”
The last surviving patient from the original AZT trial, according Burroughs Wellcome, died recently. When he died, he had been on AZT for three and one-half years. He was the longest surviving AZT recipient. The longest surviving AIDS patient overall, not on AZT, has lived for eight and one-half years.
An informal study of long-term survivors of AIDS followed 24 long-term survivors, all of whom had survived AIDS for more than six years. Only one of them had recently begun taking AZT.
In the early days, AZT was said to extend lives. In actual fact, there is simply no solid evidence that AZT prolongs life.
“I think AZT does prolong life in most people,” says Dr. Bruce Montgomery of the State University of New York at Stony Brook, who is completing a study on AZT. “There are not very many long-term survivors, and we really don’t know why they survive. It could be luck. But most people are not so lucky.”
“AZT does seem to help many patients,” says Dr. Bernard Bahari, a New York City AIDS physician and researcher, “but it’s very hard to determine whether it actually prolongs life.”
“Many of the patients I see choose not to take AZT,” says Dr. Don Abrams of San Francisco General Hospital. “I’ve been impressed that survival and lifespan are increasing for all people with AIDS. I think it has a lot to do with aerosolized Pentamadine [a drug that treats pneumocystis carinii pneumonia]. There’s also the so-called plague effect, the fact that people get stronger and stronger when a disease hits a population. The patients I see today are not as fragile as the early patients were.”
“Whether you live or die with AIDS is a function of how well your doctor treats you, not of AZT,” says Dr. Joseph Sonnabend, one of New York City’s first and most reputable AIDS doctors, whose patients include many long-term survivors, although he has never prescribed AZT. Sonnabend was one of the first to make the simple observation that AIDS patients should be treated for their diseases, not just for their HIV infection.
Several studies have concluded that AZT has no effect on the two most common opportunistic AIDS infections, Pneumocystic Carinii Pneumonia (PCP) and Kaposi’s Sarcoma (KS). The overwhelming majority of AIDS patients die of PCP, for which there has been an effective treatment for decades. This year, the FDA finally approved aerosolized Pentamadine for AIDS. A recent Memorial Sloan Kettering study concluded the following: By 15 months, 80 percent of people on AZT not receiving Pentamadine had a recurrent episode of pneumocystis. Only 5 percent of those people who did get Pentamadine had a recurring episode. “All those deaths in the AZT study were treatable,” Sonnabend says. “They weren’t deaths from AIDS, they were deaths from treatable conditions. They didn’t even do any autopsies for that study. What kind of faith can one have in these people?”
“If there’s one resistance to AZT in the general public at all, it’s within the gay community of New York,” says the doctor close to the FDA approval, who asked to remain anonymous. “The rest of this country has been brainwashed into thinking this drug really does that much. The data has all been manipulated by people who have a lot vested in AZT.”
“If AIDS were not the popular disease that it is — the money-making and career-making machine — these people could not get away with this kind of shoddy science,” says Bialy. “In all my years in science I have never seen anything this atrocious.” When asked if he thought it was at all possible that people have been killed as a result of AZT poisoning rather than AIDS he answered: “It’s more than possible.”
August 17, 1989: The government has announced that 1.4 million healthy, HIV antibody-positive Americans could “benefit” from taking AZT, even though they show no symptoms of disease. New studies have “proven” that AZT is effective in stopping the progression of AIDS in asymptomatic and early ARC cases. Dr. Fauci, the head of NIH, proudly announced that a trial has been going on for “two years” had “clearly shown” that early intervention will keep AIDS at bay. Anyone who has antibodies to HIV and less than 500 T-4 cells should start taking AZT at once, he said. That is approximately 650,000 people. 1.4 million Americans are assumed HIV antibody-positive, and eventually all of them may need to take AZT so they don’t get sick, Fauci contended.
The leading newspapers didn’t seem to think it unusual that there was no existing copy of the study, but rather a breezy two-page press release from the NIH. When SPIN called the NIH asking for a copy of the study, we were told that it was “still being written.”
We asked a few questions about the numbers. According to the press release, 3,200 early ARC and asymptomatic patients were divided into two groups, one AZT and one placebo, and followed for two years. The two groups were distinguished by T-4 cell counts; one group had less than 500, the other more than 500. These two were then divided into three groups each: high-dose AZT, low-dose AZT, and placebo. In the group with more than 500 T-4 cells, AZT had no effect. In the other group, it was concluded that low-dose AZT was the most effective, followed by high-dose. All in all, 36 out of 900 developed AIDS in the two AZT groups combined, and 38 out of 450 in the placebo group. “HIV-positive are twice as likely to get AIDS if they don’t take AZT,” the press declared.
However, the figures are vastly misleading. When we asked how many patients were actually enrolled for a full two years, the NIH said they did not know, but that the average time of participation was one year, not two.
“It’s terribly dishonest the way they portrayed those numbers,” says Dr. Sonnabend. “If there were 60 people in the trial those numbers would mean something, but if you calculate what the percentage is out of 3,200, the difference becomes minute between the two groups. It’s nothing. It’s hit or miss, and they make it look like it’s terribly significant.”
The study boasted that AZT is much more effective and less toxic at one-third the dosage than has been used for three years now. That’s the good news. The bad news is that thousands have already been walloped with 1,500 milligrams of AZT and possibly even died of toxic poisoning — and now we’re hearing that one third of the dose would have done?
With all that remains so uncertain about the effects of AZT, it seems criminal to advocate expanding its usage to healthy people, particularly since only a minuscule percentage of the HIV-infected population have actually developed ARC or AIDS.
Burroughs Wellcome has already launched testing of AZT in asymptomatic hospital workers, pregnant women, and in children, who are getting liquid AZT. The liquid is left over from an aborted trial, and given to the children because they can mix it with water — children don’t like to swallow pills. It has also been proposed that AZT be given to people who do not yet even test positive for HIV antibodies, but are “at risk.”
“I’m convinced that if you gave AZT to a perfectly healthy athlete,” says Fedorko, “he would be dead in five years.”
“This is such shoddy science it’s hard to believe nobody is protesting.”
In December 1988, the Lancet published a study that Burroughs Wellcome and the NIH do not include in their press kits. It was more expansive than the original AZT study and followed patients longer. It was not conducted in the United States, but in France, at the Claude Bernard Hospital in Paris, and concluded the same things about AZT that Burroughs Wellcome’s study did, except Burroughs Wellcome called their results “overwhelmingly positive,” and the French doctors called theirs “disappointing.” The French study found, once again, that AZT was too toxic for most to tolerate, had no lasting effect on HIV blood levels, and left the patients with fewer T-4 cells than they started with. Although they noticed a clinical improvement at first, they concluded that “by six months, these values had returned to their pretreatment levels, and several opportunistic infections, malignancies, and deaths occurred.”
“Thus the benefits of AZT are limited to a few months for ARC and AIDS patients,” the French team concluded. After a few months, the study found, AZT was completely ineffective.
The news that AZT will soon be prescribed to asymptomatic people has left many leading AIDS doctors dumbfounded and furious. Every doctor and scientist I asked felt that it was highly unprofessional and reckless to announce a study with no data to look at, making recommendations with such drastic public health implications. “This simply does not happen,” says Bialy. “The government is reporting scientific facts before they’ve been reviewed? It’s unheard of.”
“It’s beyond belief,” says Dr. Sonnabend in a voice tinged with desperation. “I don’t know what to do. I have to go in and face an office full of people asking for AZT. I’m terrified. I don’t know what to do as a responsible physician. The first study was ridiculous. Margaret Fischl, who has done both of these studies, obviously doesn’t know the first thing about clinical trials. I don’t trust her. Or the others. They’re simply not good enough. We’re being held hostage by second-rate scientists. We let them get away with the first disaster; now they’re doing it again.”
“It’s a momentous decision to say to people, ‘If you’re HIV-positive and your T-4 cells are below 500, start taking AZT,’” says the AIDS doctor who wished to remain anonymous. “I know dozens of people that I’ve seen personally every few months for several years now who have been in that state for more than five years, and have not progressed to any disease.”
“I’m ashamed of my colleagues,” Sonnabend laments. “I’m embarrassed. This is such shoddy science it’s hard to believe nobody is protesting. Damned cowards. The name of the game is to protect your grant, don’t open your mouth. It’s all about money… it’s grounds for just following the party line and not being critical, when there are obviously financial and political forces driving this.”
When Duesberg heard the latest announcement, he was partially stunned over the reaction of Gay Men’s Health Crisis President Richard Dunne, who said that GMHC now urged “everybody to get tested,” and of course those who test positive to go on to AZT. “These people are running into the gas chambers,” says Duesberg. “Himmler would have been so happy if only the Jews were this cooperative.”
* = This sentence was changed to correct an error in the original version of this article, which wrongly stated that the FDA had approved Thalidomide.
The rise and fall of AZT: It was the drug that had to work. It brought hope to people with HIV and Aids, and millions for the company that developed it. It had to work. There was nothing else. But for many who used AZT – it didn’t
RUMOURS about the drug had been circulating since early 1985 when word came from America that a company in Carolina had found a compound that was effective against HIV – at least in a Petri dish. Two years later, by the time AZT had been licensed for use, demand for it had grown to gigantic proportions.
By then, Aids patients had grown so desperate that they would sample any of the bootlegged underground therapies, some of which were probably life-threatening. With the arrival of AZT, doctors who had been powerless for so long against a syndrome about which they knew so little, at last had something they could give their patients that had passed stringent official tests.
In March 1987, when AZT was available on prescription for the first time, almost everyone with Aids wanted to take it, as did many who had tested positive for HIV. One of these was Michael Cottrell, a gay Englishman. He had tested positive for HIV in 1985 at the age of 22. He took AZT for several months in the late Eighties and suffered severe side-effects from the drug: chronic headaches and nausea, debilitating muscle fatigue. Cottrell felt much worse on AZT than he did off it. But he persevered because it seemed AZT was the only anti-Aids drug there was.
So Cottrell took it early in his infection: after all, if AZT was judged to be effective in treating Aids, then perhaps, it was thought, it would also benefit those who took it before they became ill. AZT spelt hope: psychologically it served to dispel despair. It was never claimed to be a cure, but it did claim to keep you alive longer, and in that extra time it bought, who knew what would happen? Maybe a cure would be found. Maybe a vaccine. Maybe other drugs would be developed to fight the disease, too.
Cottrell still has boxes of AZT capsules at home. He gave up on it after several months, because he couldn’t stand how ill he was feeling on the drug; he felt as though his immune system was being damaged rather than strengthened; he believed he had never encountered a drug as toxic as AZT.
Cottrell knew the drug didn’t work for him, but he believed he might have been one of the unlucky ones, like people who react badly to penicillin. Then a month ago he woke up to the news that the drug didn’t work on HIV at all, and that all his suffering had been avoidable.
Concorde, an Anglo-French programme, was the biggest clinical trial of AZT ever conducted: 1,749 patients over three years. It did not examine how effective AZT was in treating people who were seriously ill with Aids but, just as important, it looked at how effective the drug was in treating the millions of people with HIV, before they became unwell and showed Aids symptoms. Preliminary results of the trial were published in a letter in the Lancet, and made headlines worldwide. The results suggested that early intervention with AZT – for people who were HIV but had not yet developed any symptoms of Aids – was a waste of time. The study, organised by the British Medical Research Council and the equivalent body in France, reported that it made no difference to either mortality rates or disease progression if one took AZT before the onset of Aids.
In a ‘blind’ test, AZT was given to 877 people and 872 were given a placebo. As soon as a patient developed any Aids symptoms, he or she (15 per cent were women) would be offered ‘open-label’ AZT. The mortality rates appeared to be shocking: over the three years of the trial, there were 79 Aids-related deaths in the AZT group, but only 67 in the placebo group. The researchers explained that among so many patients this figure was not statistically significant, but if you were HIV-positive and read of this in the newspapers, you were bound to question all the great claims that had been made for AZT. More people got Aids and died on Concorde than on any previous trial.
There were other causes for concern. Those on AZT developed more side-effects than those on the placebo. The results of the tests also cast doubt on one of the fundamental ways we measure a person’s immunity to disease. Those given AZT early increased their ‘CD4’ or ‘T4’ cell count; these are the cells attacked by HIV, and their numbers drop as the disease spreads. But the fact that, even with this higher count, patients did not live longer or develop the disease more slowly, struck at one of the basic tenets of Aids research.
Cottrell told the news to his 28-year-old partner Karl Burge, who had been diagnosed as HIV-positive four years ago, and they decided to take action. But what could they do? They had already joined protests against Wellcome plc, the British company that made AZT and had reaped millions in sales and share profits. Wellcome executives had listened to their complaints, and had admitted to certain levels of toxicity in AZT, but claimed that their product still had great beneficial effects. They were not readily going to halt production of the drug that last year made them pounds 213m, their second biggest earner.
So Cottrell and his friends selected a new target, the Terrence Higgins Trust. This was a strange choice: the trust, Britain’s most prominent Aids charity over the past 10 years, is staffed by dedicated professionals and volunteers providing a large range of support and information about all aspects of Aids and HIV; it developed the caring ‘buddy’ system; it produced information for schools; it sat on many Aids research panels and often met government departments.
So what had it done wrong? It had taken money from Wellcome plc and included positive information about AZT in its many leaflets and documents. Cottrell and his friends felt they were being betrayed by the very organisation that they had believed existed to act in their best interests; they felt that what was once an invaluable institution was acting as a mouthpiece for a multinational pharmaceuticals company.
Last week, Cottrell and Burge were still pitched outside the Terrence Higgins Trust office in central London, four weeks after their protest began. On Wednesday they were arrested and charged with a public order offence after a member of the trust called the police. The protest is growing by the week. They have been joined by John Stevens, diagnosed HIV- positive more than eight years ago, and who also had bad experiences with AZT, and Pierre Hardy, diagnosed HIV-positive four years ago when he was 27 and had felt devastated by its effects. Many other protesters carry placards, collect signatures, hand out leaflets. You will not find a more potent symbol of the complex story of AZT, a story of how the struggle to find a ‘magic bullet’ to help millions of people has degenerated into a saga of distrust, confusion, and anger. It is a story of health and illness, but it is also a story of scientific ambition, secrecy and political pressure, and of the amounts of money that can be generated when a lethal virus turns into a worldwide epidemic.
IN 1964, Jerome Horwitz was working in his laboratory at the Michigan Cancer Foundation when he had what he hoped was a brilliant idea. At 45, Dr Horwitz was the foundation’s director of chemistry, and although not in the scientific premier league, was a respected local researcher with his own lab and assistants. He had spent much of the previous decade doing what many of the world’s leading scientists had done – working on a cure, or at the very least an effective treatment, for cancer.
He developed a theoretical solution: what was needed was a chemical that would insert a ‘phoney’ compound into the DNA ‘building block’ of a cell to prevent its replication. After years of research, Dr Horwitz came up with
azidothymidine (AZT).
He tried his new compound on leukaemic mice, but it had no effect. Horwitz didn’t know why, but AZT didn’t work.
Horwitz never became famous. Recently he said AZT ‘was a terrible disappointment . . . we dumped it on the junkpile. I didn’t keep the notebooks.’ The compound remained ‘on the shelf’, occasionally tried by other researchers but always found to be useless. There was no reason to patent it. But 20 years later, Burroughs Wellcome brought it back to life.
THE WELLCOME group was founded in London by two Americans in 1880. Its first significant achievement was the creation of the tablet – previously most medication had been administered in powder form. In the 1930s the group was split into two distinct parts: the Wellcome Trust, a large charity which devoted its income to scientific research and the maintenance of an institute and library concerned with the history of medicine; and the Wellcome Foundation Ltd, a profit-making pharmaceuticals company that was called Burroughs Wellcome in the United States. In the course of its research, Wellcome employees have won five Nobel prizes.
By 1980, Wellcome had specialised in the treatment of viruses for more than 15 years, and its anti-viral drugs accounted for the bulk of its income. In that year, David Barry, a leading researcher at Burroughs Wellcome in the US, noticed that demand for its drug Septra – a drug that Wellcome had helped to develop a few years earlier to combat a rare form of pneumonia – was suddenly on the increase. Previously this pneumonia, known as PCP, was prevalent only in children with leukaemia, but now many doctors were requesting it for adult males. Most of these men were gay, and living in New York and San Francisco.
Two years later, another new Wellcome drug, Zovirax, was in great demand among the same group of people. Zovirax was an anti- herpes treatment. Dr Barry was very disturbed by the sudden demand for these two drugs.
Aids (Acquired Immune Deficiency Syndrome) was first classified as a new disease in 1981, but it was not until 1984 that the cause was identified as HIV (Human Immunodeficiency Virus). This cause has since been challenged by several prominent molecular biologists, but it remains the cornerstone of Aids research. And if any company was ideally equipped to conduct research into combating a new virus, it was Wellcome.
It was only natural for Barry to devote much of the company’s research resources to fight HIV. No one knew how widespread the virus or Aids was or would become. In 1984, only about 3,000 people had been diagnosed with Aids, but some early forecasts were terrifying: millions of people might already be infected, and hundreds of thousands could die within the next few years. Any scientist could see that Aids was potentially a career-making race to the Nobel prize. Millions might be made from a successful treatment.
After a few years of government inactivity – shameful years in which this new disease was virtually ignored – political ambition added to the desire to find a treatment. Health departments noticed that it wasn’t just homosexuals who were being struck down, but also hundreds of haemophiliacs and drug users. A certain amount of official panic took hold: by the time Rock Hudson died in the summer of 1985, it was clear that anyone – even film stars – could be in the frontline.
According to Wellcome’s own three-page account, research into HIV began in June 1984. During mass testing of scores of anti-viral
compounds, a substance known at first only as Compound S was found to inhibit viruses in animal cells. Compound S was AZT, a resyn- thesised version of what Horwitz had made 20 years before (Wellcome credits Horwitz in its account, but spells his name wrong).
In November 1984, according to the Wellcome account, the company sent samples of AZT to Duke University in North Carolina, the Food and Drug Administration (FDA) and the National Cancer Institute for independent testing, and within a few weeks the results confirmed what Wellcome already believed: that the stuff worked against HIV in test-tubes under laboratory conditions. Wellcome had already progressed further than Horwitz, but the real test – its effect on humans – was fraught with danger.
But first there is another account of the development of AZT to consider. A US government official named Sam Broder believes he has far more claim to being ‘Mr AZT’ than anyone at Burroughs Wellcome. Broder, the director of the National Cancer Institute, claims that Burroughs Wellcome showed little interest in developing an anti-Aids drug.
Broder went on a tour of pharmaceuticals companies towards the end of 1984, imploring them to send any possible anti-viral compounds to his lab for testing in safe conditions. ‘I went to one prestigious company, hat in hand,’ he told the business writer Bruce Nussbaum, whose book, Good Intentions, traces a history of the search for anti-Aids drugs. ‘I got about one minute and thirty seconds of a high-ranking officer’s time. It was very disappointing for me. It was emblematic of the issue. There was no real interest in it.’
Broder then went to Burroughs Wellcome. He says: ‘They made it clear that on the basis of 3,000 patients, there was no way they could practically get involved.’ Broder says he then became abrasive. ‘As I left, I said, ‘You know, we’re going to have more than 3,000 cases. It is going to be commercially viable for you . . .’ ‘
Whoever pushed who, the drug came through. When Broder found that the AZT sent to him by Burroughs Wellcome in November 1984 worked against the virus, he assured the company that every effort would be made to get this great new drug to dying patients as soon as possible. The FDA’s stringent testing requirements mean that most new drugs take between eight and 10 years to pass from development to the marketplace. AZT was pushed through in just 20 months.
This could have been the early history of almost any drug; the difference is, during what would normally have been an eight-year test period, for six of those years the drug was already on the market. At a time of desperation, this drug looked like the one that would restore hope. The National Cancer Institute had previously tried one other therapy, Suramin, which proved to be toxic in early tests, but AZT appeared to be far less poisonous. And so it was put on the ‘fast track’: the testing of some other drugs for less life-threatening illnesses was put aside; AZT was given top priority, an all-or-bust thing. But could any drug live up to the boundless hopes pinned on AZT?
THIS IS how AZT is supposed to work against HIV. HIV enters body cells, usually T4 white blood cells that play a crucial role in the orchestration of the body’s immune system. HIV is one of a group of viruses known as retro- viruses, which means that, unlike most living things that store their genetic information as DNA, HIV stores it as RNA. Before HIV can replicate, it must convert its RNA code to DNA by use of a special enzyme. It is during this conversion process that AZT works. When AZT enters the body, it is transformed into a molecule that closely resembles one of the building blocks of DNA. During the process of HIV conversion, this molecule is incorporated mistakenly into the DNA. The addition of this ‘phoney’ molecule makes the addition of further building blocks impossible and halts replication of the virus. It’s a form of chemotherapy. It worked fine under a microscope.
The first human tests were in two phases. The first examined whether AZT could be tolerated in the body at all, and whether it entered the brain, crossing the ‘blood-brain barrier’; to know this was important, because a common Aids symptom is dementia. The first Aids patient was injected with AZT in July 1985. This test concluded that the blood-brain barrier was crossed, and that although there were levels of toxicity detected, these were deemed to be safe.
The second phase of the tests, the final hurdle to the granting of a licence for mass production, was a shambles. It was set up six months later to establish whether AZT would combat Aids. This test, overseen by the Food and Drug Administration, involved 282 patients, all of them already ill with Aids or Arc (Aids-related complex). It was to be a placebo test, conducted over 24 months. It was to be a ‘double-blind’ study in which neither patient nor doctor knew whether the capsules being taken were AZT or starch. (But before the tests could begin, Wellcome had to produce large quantities of AZT, and found it couldn’t do it. It had run out of one crucial ingredient: herring sperm. Finally, Wellcome bought it in bulk from another company.)
At a press conference after the tests in September 1986, Wellcome reported that they had been a considerable success, such a success that the 24-week trial had been halted after 16 weeks for ‘ethical’ reasons. Mortality rates for people taking AZT were staggeringly lower than those taking the placebo; there had been 19 deaths in the placebo group of 137 people, but only one in the AZT group of 145. Those on AZT also had a decreased number of opportunistic infections and showed improvement in weight gain and T4 cell counts. Wellcome agreed in response to pressure from some sectors of the gay community that if AZT was effective, then dying people should be taken off the placebo at once.
No one claimed it was a cure, but there was huge relief that a breakthrough had been made. There had been much embarrassment when it became known that Rock Hudson had attended the Pasteur Institute in France for treatment; now at last America was showing those foreigners a thing or two. Robert Windom, assistant health secretary, said that ‘treatment with AZT prolongs survival of persons with Aids’. The results were ‘exciting’.
It was not suitable for everyone, but it was the best thing yet. In fact, it was the only thing. Last year, interviewed in the Wellcome in- house magazine, David Barry said that ‘the staff at Wellcome can tell our children, grandchildren and great-grandchildren that we were there, that we made a difference’. When it was shown that AZT worked, ‘we . . . first had a frenzied, cheerful celebration, and then a very quiet one. The longer we considered the global implications, the greater the accomplishment we realised Wellcome had made in the control of the HIV epidemic.’
But a few months after AZT was made available, John Lauritsen, a journalist working on the gay newspaper New York Native, obtained test documents through the Freedom of Information Act that suggested that many rules had been broken in the trials. The trial had been ‘unblinded’ within weeks: some patients claimed they could tell what they were taking by taste; others were so keen to have AZT that they pooled their treatment with other patients to increase their chances of receiving the drug. The documents showed that almost half the AZT patients had received numerous blood transfusions in the course of the trial, because of damage to their bone marrow and immune systems; and that a few had to be taken off AZT altogether.
What happened after the trial ended suggested something more alarming about AZT. After 16 weeks, one AZT patient was dead, compared to 19 placebo patients; a week later two more patients on AZT had died, compared to four more on the placebo. The ratio had switched from 19:1 to 23:3, which suggested AZT might only be effective for a limited time.
If the trial had continued, the ratio might have narrowed even more. The tests would probably still have shown that AZT has some benefits for very ill patients, but with hindsight it is alarming that a new drug was allowed to be
released with so much left to prove. People at Wellcome now put it down to the mood and the severe pressure of the times. Dr Trevor Jones, Director of Research at Wellcome, who has been involved in their development of AZT from the beginning, acknowledged that the trials were subject to extraordinary pressures. ‘Much of these accusations (about the breakdown of trial protocol) took place, not at that stage, but later on, when the drug was showing benefit in a less sick population.
All sorts of things we heard stories about, and some of them I think we can confirm from our data. Patients would go to their doctor, get their treatments, and rather than risk the uncertainty (or receiving the placebo), they’d put the two together, mix them and divide them by half. We know this, because people who were supposed to be on the placebo already had drug levels in them.’
Much of the pressure came from people with HIV and Aids, and their carers, who wanted the drug released immediately. It was unacceptable to administer a placebo, they argued, if AZT worked. And there was no point having a drug released on the market in 10 years – by that time hundreds of thousands would be dead.
Burroughs Wellcome and many other independent research institutions would spend every subsequent year trying to supplement their data on AZT, trying to find out all the things that would normally be known about a drug before it hit the market. In these later years AZT was to become for many people the symbol of all that was wrong with Aids research. Once AZT was shown to have worked, almost all available funds were channelled to support its development and other potential treatments, along with any doubts that HIV was the cause of Aids, were swept aside.
BUT IN 1986, AZT was unstoppable. It suited the FDA, because it showed the administration was doing something. It suited Wellcome, because it now had a patent on AZT (and by 1986, with the epidemic increasing alarmingly, there was no doubt that the financial rewards would be enormous). It suited doctors, because they believed they could help their patients. And it certainly suited people with Aids. Some people had doubts, but hell, if you were ill and dying you wanted to believe. After all the despair and uncertainty, people in authority were saying ‘take this, it’ll do you good’.
Cottrell was one of the first people to take AZT in Britain. He was prescribed it in 1986, before it was widely available, when he was 23.
‘I had recently been diagnosed HIV-positive, and I went into a panic. I thought I was going to die. I remembered something about this drug coming from America and everyone clamouring to get it. I was perfectly healthy. My boyfriend’s blood count was quite low, and he was prescribed it by St Stephen’s Hospital, and I took it too. Intuitively, I didn’t think it was doing me any good. I was prescribed it three times over a period of three years, and I took it out of fear. I was first prescribed 1,200mg a day, and then 500mg, but I still felt bad, even on the lower dose. I had nausea and headaches and muscle fatigue.’
Cottrell took it every four hours, which meant he had to have a bleeper that woke him at three or four o’clock every morning. (People joked that the real Aids money lay in making these bleepers; in New York in the late Eighties, opera performances were punctuated by bleeps.) Cottrell stopped taking AZT after a few weeks, but then he got scared, and began taking it once more. ‘I got my drugs every two weeks – a big plastic bagful. I felt that I was carrying my life around in that bag.’
His friend, Pierre Hardy, was diagnosed HIV in 1989, when he was 28. At a specialist clinic he was given a sheet of paper which explained that AZT was the most efficient treatment, but also that it hadn’t been around long enough for anyone to know the long-term effects. Like most people in his position, he said he’d try anything, and he was prescribed 500mg a day.
‘My T4 count went up along with my general health in the first year, and everything settled down. I had been on AZT for three years, and my T4 count was levelling between 400 and 600 (an average T4 count in healthy adults is between 800 and 1,000). And then last year I started to get sick. I had repeated chest infections, and in November 1992 I had a stroke. I was hospitalised in a specialist ward. I asked them for my T4 count, and when they came back, they were were uncomfortable about it. My T4 count was 90. I thought I was finished.
‘When I got home and started to review the whole thing, the whole HIV theory. I threw away all the pills I was taking – I was taking seven every morning and evening. I started to change my diet, and then I went back to my doctor. When I had my new T4 count it was 545. I’ve had three migraines since January, a little bit of asthma coming back, but basically I feel much better. If I’d continued to believe in the traditional medicine sytem I would have been dead either this year or next year.’
Two weeks ago Hardy met a volunteer with the Terrence Higgins Trust, who told him that he and his boyfriend were taking AZT and it was working like a dream.
‘I asked him how long they were on it. He said four months. I said that that was the trap that everyone was falling into. The AZT will work for you for a little while, for the maximum of one year, as it did for me, and afterwards the damage became visible.’
Most people with Aids, and many with asymptomatic HIV, take or have taken AZT. Other drugs have emerged in the past few years that work in a similar way – DDC (produced by the Swiss company Hoffmann-La Roche) and DDI (made by the American company Bristol-Myers Squibb), but AZT is still the market leader. It is hard to think of another product that is so dominant in its field. You read the showbiz autobiographies and those three little letters snap out of the page.
Earvin ‘Magic’ Johnson, the basketball star who tested HIV-positive in October 1991, was advised to take AZT immediately. He agreed. ‘There was a lot of public interest in the fact that I was taking AZT, which was originally used only in the later stages of the illness,’ he explained in My Life, his autobiography. ‘These days it’s used as a preventative, but not everybody knew that. That may be why some people, including a few reporters, concluded that I was sicker than I actually was.’ People wrote to Johnson telling him that AZT was not the answer. Somebody advised him to drink all his blood and replace it with new blood. ‘Even now I can’t go anywhere without somebody coming up and saying, ‘I know this friend who knows this doctor who has a cure’.’
Rudolf Nureyev, who died in January, began taking AZT in 1988. ‘AZT was just beginning to be used in France,’ said Michel Canesi, his doctor. ‘I didn’t want to give it to him straight away, because I was worried that the side-effects would hamper him (Nureyev was still dancing at this time). Rudi lost his temper and said: ‘I want this medicine.’ I replied that there hadn’t been long enough to judge the results. But I had to give in and prescribe it – he was so insistent. But he didn’t take it regularly. He went off every time with tons of drugs, and every time I went to see him I found unused packets all over the place.’
The film-maker Derek Jarman, who was diagnosed HIV-positive in 1986, has found AZT beneficial. ‘It works – it holds everything up. It stops the virus replicating. At the beginning they gave people much too massive doses, which affected us physically. I had no recognisable toxic side-effects from it. I began taking it in September 1990, I think, and I came off it last August.
‘I was invited by my doctor to make up my mind whether I took the drug or not, so I rang up various people in America and the general advice was to take it – and this was advice was from quite radical people, not people in with the Wellcome Foundation.
‘I came off it because my doctor said that my (T4) count was down. We’ve never discussed it since. He just suddenly said, ‘I think you’ve had enough AZT, Derek’, and I very much trust him, he’s a brilliant doctor. The whole thing is so complicated, because I took a lot of other drugs as well. I had to have suppressants for TB, toxoplasmosis and PCP. And then obviously if I got an infection there was fluconazole and all of that area. And then at a certain point they added hydrocortisone and fludrocortisone to keep my energy up.’
Jarman has recently been in hospital. ‘At the moment I’m actually on nothing. I’ve had a skin complaint and they decided it would be very sensible to take me off all my pills, and then go back on the drugs to see if they were causing the skin complaint. They can obviously play around with the drugs.
‘My feeling about AZT is that I’m glad I took it, even though I can’t prove to you that it did anything. You can say that if it helps someone psychologically then it must be doing some good. I think the doctors generally feel that it does some good. But how do you know?’
FINANCIALLY, Wellcome plc has done extremely well out of AZT. Retrovir, the drug’s brand name, accounts for more than 13 per cent of its total income, and yielded pounds 213m last year. As the only big earner to have been launched by the company in the past decade, the continued success of AZT is crucial to its growth. The company will be well aware that at the end of last year the World Health Organisation estimated that about 13 million men, women and children have been infected with HIV since the start of the pandemic. (A large proportion of these cases are in sub-Saharan Africa and South and South-east Asia, where AZT and other anti-Aids treatments are unlikely to be available or affordable; the figure for HIV infection in the Americas and Western Europe is estimated at 2.5 million.)
Part of the Wellcome Foundation was floated on the stock market in 1986, the year of the AZT breakthrough. Subsequent rises in share prices have been directly linked to the fortunes of the drug and the results of new trials. In February 1987, the share price jumped 73.5p to 374.5p on the news that AZT would be widely available in the US at dollars 188 for 100 capsules, an extremely high price for a new drug, and one that would yield large profits (this translated to about dollars 10,000 a year for every user). By November 1989 the share price had almost doubled to 724p; year-on-year pre-tax profits were up 28 per cent to pounds 283m. In early 1993, the share price was at 810p; last year’s pre-tax profits were pounds 505m.
‘In terms of the emotive quality of the demand, there’s never been a drug like it,’ said Martin Sherwood, a Wellcome spokesman, shortly after AZT’s launch. It was just this emotive demand that led to the picketing of the Wellcome shareholders’ meeting in January 1990. Act Up (the Aids Coalition to Unleash Power, co-founded by the playwright Larry Kramer) picketed the AGM at Grosvenor House in London, describing it as ‘a gathering of Aids profiteers’. Activists complained about the price of AZT, and what they saw as Wellcome’s reluctance to provide all available information on the drug.
Wellcome shareholders were irritated by this intrusion, not least when Act Up members interrupted the meeting and insisted on talking to Sir Alfred Shepperd, the outgoing chairman. But Wellcome executives were baffled: they believed they had done everything they could to benefit people with HIV and Aids, certainly more than any other pharmaceuticals company. Was it not these very same activists who had celebrated when AZT was launched three years earlier? At first Wellcome defended its pricing on the grounds that AZT took dollars 80m to develop and produce (later revised to dollars 30m), but it soon bowed to pressure (and its economies of scale) and cut the price. The recommended dosage was also reduced for medical reasons, which meant many more people could tolerate its toxicity. Today AZT costs about dollars 3,000 per person per year, or about pounds 2,000.
As would be expected, Wellcome plays up the good news. When, in 1989, two double- blind placebo trials of the effects of AZT on asymptomatic and less seriously ill patients showed that it could delay the progression of the disease, much was made of the results and the share price rose by 30p. But when, four months later, the company admitted that AZT had caused cancer in rodents, it explained that the rats and mice were given 10 times the dose prescribed to humans, and that several other drugs in use by humans had also produced tumours in animals when administered over long periods. Wellcome’s share price went down one penny.
Wellcome’s PR machine is an impressive force, and much money is spent on convincing the media of AZT’s worth. You go and see them and you get a lot of bumph: how AZT works, why it is more effective than other anti- retrovirals. Wellcome house-magazines talk of the extra 400,000 productive years of life it has made possible through the drug, about how many thorough and independent studies have stressed AZT’s efficacy.
‘The number of people who have shown agression against us concerns us no end,’ says Trevor Jones. ‘Normally the company tries to distance itself from the patient / physician interaction – it must do. The day-to-day therapy of the patient is not our responsibility. But about three years ago we started to open our labs to people with HIV and their carers, contrary to the advice of my security and other colleagues. You then realise the uncertainty and the frustrations involved in that act of taking a tablet for the very first time. When people with HIV came through the door of the lab I could almost touch their anger. But I realised that the anger was not really about Wellcome or me, but about their mortality. They were frustrated, and saying, ‘Please, please what can I do?’ These were genuine cris de coeur.’
Dr Jones is one of the few pharmaceutical industry representatives on Britain’s Medical Controls Agency. Wellcome has clearly selected its spokesman with care. ‘People say we’re purely acting out of commercial interests, but it is not in our commercial interests to do anything else but get this drug right,’ Dr Jones says. ‘We wanted to show people that we are working night and day, weekdays and weekends trying to develop better medicines. Otherwise we look like ogres and robber barons all the time. That’s the whole history of our business; if you’ve got a problem with a product, you must, you must, you must tell people. The criticism hurts a lot; our integrity as a scientific body is important to us. I don’t take too kindly to people saying, ‘Oh, you don’t want to listen to Wellcome, because they would say that, wouldn’t they?’ You can’t hide anything in this business, because otherwise who will trust us when we develop another drug, like the new epilepsy drug we’ve got now? You have to believe that the integrity of science is good.’
Jones has had a bad few weeks. Wellcome’s share price was hammered by last month’s Concorde trial report, falling 10 per cent to 670p, before rallying to 692p. Five days after the report appeared, Wellcome staged a damage limitation exercise, at which Jones told a press conference that he was unhappy with the way the results were released, without peer review or advice to patients, and saying it had caused panic among those with HIV. He said that the full results had yet to be released, and hoped that a more beneficial picture of early intervention with AZT would emerge at the ninth International Aids Conference in Berlin in June. He also outlined that the protocol of the study had changed from that agreed in 1988. When an American study reported in 1989 that AZT did have beneficial effects on people with asymptomatic HIV, the Concorde officials decided that people on its trial could switch to AZT if they wanted to; this may have led to a diluting of the results.
Last week, Jones reiterated why AZT may still be beneficial, and why doctors should continue to prescribe the drug early. ‘We have gathered together 10 studies on asymptomatic patients. Five of these are control studies with placebos, and five are cohort studies, in which we simply give the drug and observe what happens. These studies involved more than 6,500 patients and ranged from one to four years in duration. We believe we have accrued sufficient data to show that taking the drug when you’re asymptomatic does delay the onset of further symptoms.’
WELLCOME has a presence at all the chief Aids conferences, and will occasionally organise gatherings of its own. In June 1992 it launched Positive Action, ‘an international intiative’ in support of those with HIV and Aids. For the launch conference in London, journalists flew in from all over Europe to hear Wellcome executives describe how pounds 1m was being distributed to many educational organisations. An emotional climax of sorts was provided by Jerry Breitman, the company’s US director of professional relations. He was there to present the ‘workplace initiative’, and his speech contained a little surprise at the end. Like the wig salesman whose coup de grace is to rip off his own toupee, Breitman declared himself HIV-positive. ‘I thought long and hard before deciding to tell my management,’ he revealed. ‘But . . . when you are part of an enlightened organisation such as Wellcome, I am absolutely convinced that communicating your HIV infection is a positive action . . . It is, truly, one of the best decisions I have made in a very long time.’ A few journalists felt distinctly queasy at the theatricality of it all.
One of the initiatives raised was Wellcome’s involvement with the Terrence Higgins Trust. This first surfaced in 1991, with the publication of four information leaflets. Two months ago staff at the Trust and volunteers read in their newsletter that the link had been strengthened. The newsletter explained that ‘THT, along with the Wellcome Foundation, is about to begin producing an important new medical information series. THT are providing a series of medical updates for all staff and volunteers. We will be providing them on a regular basis every two months in the evening. Costs will be met by the Wellcome Foundation, which also funds our series of general booklets.’
Nick Partridge, chief executive of the trust, is dubbed ‘Nick the Sick’ on the placards carried by the protesters outside his office. Partridge, in reply, calls them ‘New Age flat- earthers who have a naive hope that Holland & Barrett will produce a herbal tea that will be effective against HIV.’ Partridge said that the trust actively pursued funding from a wide range of companies and government agencies, and that it was ‘quite clear that none of that funding involves an ability by those companies to influence the information we produce. We would be neglecting our duty if we were not in regular contact with Wellcome, Bristol-Myers Squibb and Roche, arguing for greater investment in HIV research and fair and balanced information. The leaflets are not about treatment issues.’
But once they were. In 1991 the trust produced a 24-page booklet on HIV and its treatment; nine pages were devoted to AZT, but only half a page was given to other therapies. The copyright on the leaflet was held by the Wellcome Foundation, which also paid for its printing. ‘It was only available for eight months,’ Partridge says. ‘Information changes quite rapidly. The main fault of that leaflet is that it is too hopeful. By 1991 the hopes around early intervention had probably gone further than we realise, in retrospect, was wise. The desire by many people with HIV to say, ‘Yes, we can live with this infection’ meant that a lot of hope was invested in the theory of early intervention. For all its faults, our leaflet was still a lot more realistic than the material that Wellcome was putting out on its own. Remember that over the years, there have been many stories of breakthroughs that proved to be wildly optimistic.’
FOR MOST people with HIV, the AZT dream is over. AZT is the future that was; no one believes in the ‘magic bullet’ any more. It does have benefits for some patients who are seriously ill, but there is now severe doubt over its other uses. This, after the drug has been subjected to more tests, and has been the subject of more post-launch research papers, than perhaps any other modern therapy.
The future for HIV and Aids treatment appears to be in combination treatment – the use of AZT and DDC and DDI and many other compounds used in all manner of variations. Several trials are in progress. Two weeks ago it was announced that Wellcome has joined forces with its competitors Hoffman-La Roche, Bristol-Myers Squibb, Glaxo, SmithKline Beecham and 15 other companies, in an attempt to pool their research knowledge and find an effective treatment.
Wellcome is also developing some other anti-Aids drugs on its own. We won’t hear about these for a while; the company doesn’t want to raise any hopes.
Jerome Horwitz, the man who created AZT in 1964, is still active in medical research. He’s 74 now, but you can still reach him most days at the Meyer L Prentis Cancer Center in Detroit. Occasionally he does a little Aids work, but most of his time involves cancer chemotherapy.
Horwitz believes AZT is not the answer to HIV and Aids, but has hopes for combination therapies (he was also the first to synthesise DDC). He concludes that AZT ‘buys time’.
‘We were certainly on the cutting edge,’ he says of his work in the mid-Sixties. ‘When the pharmacologist said, ‘Look, Dr Horwitz, your compounds are not effective against leukaemias and I see no future for them’, that was like a blow to the solar plexus. We had great hopes. ‘I remember one of my students saying at the time that we had a great series ofcompounds just waiting for a disease totreat. It took 25 years before our beliefs were vindicated.’
The first Horwitz heard of AZT’s use against HIV was when he read about it in the Wall Street Journal. Burroughs Wellcome established a chair in his name at the Michigan Cancer Foundation, but he has received no financial reward.
‘My wife sits across from me at the
breakfast table and reminds me of all the
money that Burroughs Wellcome has got out of it and I haven’t got a dime. I keep telling her about the legacy I’m leaving. But I wouldn’t be being absolutely straight with you if I hadn’t thought that I should have gotten something out of it.’-
Although we often speak of “the Buddha,” there are many Buddhas in Buddhism. On top of that, the many Buddhas come with many names and forms and play multiple roles. The word “Buddha” means one who woke up,” and in Buddhist doctrine, any such enlightened individual is technically a Buddha. In addition, the word Buddha is often used to mean the principle of Buddha-nature. But of course, there is one historical figure that normally is considered the Buddha.
Shakyamuni Buddha is a name given to the historical Buddha, especially in Mahayana Buddhism. So it’s nearly always the case that when someone is talking about Shakyamuni, he or she is speaking of the historical figure who was born Siddhartha Gautama but then became known as Shakyamuni only after he became the Buddha. This person, after his enlightenment, is also sometimes called Gautama Buddha.
However, people also speak of Shakyamuni as a more transcendent figure who still is, and not as a historical figure who lived a long time ago. Especially if you are new to Buddhism, this may be confusing. Let’s take a look at Shakyamuni Buddha and his role in Buddhism.
The Historical Buddha
The future Shakyamuni Buddha, Siddhartha Gautama, was born in the 5th or 6th century BCE in what is now Nepal. Although historians believe there was such a person, much of his life story is shrouded in legend and myth.
According to legend, Siddhartha Gautama was the son of a king, and as a youth and young adult, he lived a sheltered and pampered life. In his late 20s, he was shocked to witness sickness, old age, and death for the first time, and he was filled with such dread he resolved to give up his royal birthright to seek peace of mind.
After several false starts, Siddhartha Gautama eventually settled determinately into deep meditation under the famous Bodhi tree in Bodh Gaya, in North Eastern India, and realized enlightenment, at about the age of 35. From this point on he was called the Buddha, which means “one who woke up.” He spent the rest of his life teaching and died at about the age of 80, achieving Nirvana. More detail about the life of the Buddha can be read in The Life of the Buddha.
About the Shakya
The name Shakyamuni is Sanskrit for “Sage of the Shakya.” Siddhartha Gautama was born a prince of the Shakya or Sakya, a clan who appear to have established a city-state with a capital in Kapilavatthu, in modern-day Nepal, about 700 BCE. The Shakya were believed to have been descendants of a very ancient Vedic sage named Gautama Maharishi, from whom they took the name Gautama. There is a bit of legitimate documentation of the Shakya clan that can be found outside of Buddhist texts, so it appears the Shakya was not just an invention of Buddhist story-tellers.
If indeed Siddhartha was the heir of the Shakya king, as legends suggest, his enlightenment may have played a small role in the clan’s downfall. The Prince had married and had fathered a son before he left his home to seek wisdom, but the son, Rahula, eventually became his father’s disciple and a celibate monk, as did many young men of the Shakya nobility, according to the Tipitaka.
Early scriptures also say the Shakya and another clan, the Kosala, had long been at war. A peace agreement was sealed when the Kosala crown prince married a Shakya princess. However, the young woman sent by the Shakya to marry the prince actually was a slave, not a princess–a deception not discovered for a long time. The couple had a son, Vidudabha, who swore revenge when he learned the truth about his mother. He invaded and massacred the Shakya, then annexed Shakya territory into Kosala territory.
This happened near the time of the Buddha’s death. In his book, Confessions of a Buddhist Atheist Stephen Batchelor presents a plausible argument that the Buddha was poisoned because he was the most prominent surviving member of the Shakya royal family.
The Trikaya
According to the Trikaya doctrine of Mahayana Buddhism, a Buddha has three bodies, called dharmakaya, Samb Hoga kaya, and Nirvana kaya. The Nirvana kaya body is also called the “emanation” body because it is the body that appears in the phenomenal world. Shakyamuni is considered a Nirvana kaya Buddha because he was born, and walked the earth, and died.
The samghogakaya body is the body that feels the bliss of enlightenment. A Samb Hoga kaya Buddha is purified of defilement and is free of suffering, yet maintains a distinctive form. The dharmakaya body is beyond form and distinction.
The three bodies actually are one body, however. Although the name Shakyamuni usually is associated with the Nirvana kaya body only, occasionally in some schools Shakyamuni is spoken of as all bodies at once.
Queen Maya’s retreat to Lumbini to gave birth to Prince Siddharta Gautama (Buddha), the panel of Lalitavistara, Borobudur, Central Java, Indonesia. Gunawan Kartapranata/Wikimedia Commons
Aspects of the story of Buddha’s birth may have been borrowed from Hindu texts, such as the account of the birth of Indra from the Rig Veda. The story may also have Hellenic influences. For a time after Alexander the Great conquered central Asia in 334 BCE, there was a considerable intermingling of Buddhism with Hellenic art and ideas. There also is speculation that the story of the Buddha’s birth was “improved” after Buddhist traders returned from the Middle East with stories of the birth of Jesus.
The Traditional Tale of the Buddha’s Birth
Twenty-five centuries ago, King Suddhodana ruled a land near the Himalaya Mountains.
One day during a midsummer festival, his wife, Queen Maya, retired to her quarters to rest, and she fell asleep and dreamed a vivid dream, in which four angels carried her high into white mountain peaks and clothed her in flowers. A magnificent white bull elephant bearing a white lotus in its trunk approached Maya and walked around her three times. Then the elephant struck her on the right side with its trunk and vanished into her.
When Maya awoke, she told her husband about the dream. The King summoned 64 Brahmans to come and interpret it. Queen Maya would give birth to a son, the Brahmans said, and if the son did not leave the household, he would become a world conqueror. However, if he were to leave the household he would become a Buddha.
When the time for the birth grew near, Queen Maya wished to travel from Kapilavatthu, the King’s capital, to her childhood home, Devadaha, to give birth. With the King’s blessings, she left Kapilavatthu on a palanquin carried by a thousand courtiers.
On the way to Devadaha, the procession passed Lumbini Grove, which was full of blossoming trees. Entranced, the Queen asked her courtiers to stop, and she left the palanquin and entered the grove. As she reached up to touch the blossoms, her son was born.
Then the Queen and her son were showered with perfumed blossoms, and two streams of sparkling water poured from the sky to bathe them. And the infant stood, and took seven steps, and proclaimed “I alone am the World-Honored One!
Then Queen Maya and her son returned to Kapilavatthu. The Queen died seven days later, and the infant prince was nursed and raised by the Queen’s sister Pajapati, also married to King Suddhodana.
Symbolism
There is a jumble of symbols presented in this story. The white elephant was a sacred animal representing fertility and wisdom. The lotus is a common symbol of enlightenment in Buddhist art. A white lotus, in particular, represents mental and spiritual purity. The baby Buddha’s seven steps evoke seven directions—north, south, east, west, up, down, and here.
Buddha’s Birthday Celebration
In Asia, Buddha’s birthday is a festive celebration featuring parades with many flowers and floats of white elephants. Figures of the baby Buddha pointing up and down are placed in bowls, and sweet tea is poured over the figures to “wash” the baby.
Buddhist Interpretation
Newcomers to Buddhism tend to dismiss the Buddha birth myth as so much froth. It sounds like a story about the birth of a god, and the Buddha was not a god. In particular, the declaration “I alone am the World-Honored One” is a bit hard to reconcile with Buddhist teachings on nontheism and anatman.
However, in Mahayana Buddhism, this is interpreted as the baby Buddha speaking of the Buddha-nature that is the immutable and eternal nature of all beings. On Buddha’s birthday, some Mahayana Buddhists wish each other happy birthday, because the Buddha’s birthday is everyone’s birthday.
Reference
O’Brien, Barbara. “The Birth of the Buddha.” Learn Religions, Feb. 11, 2020, learnreligions.com/the-birth-of-the-buddha-449783.
For years, Rosemary Kennedy’s story was kept secret after her lobotomy was botched, leaving her unable to walk or talk.
The Kennedy Family at Hyannis Port on September 4, 1931. From left to right: Robert, John, Eunice, Jean (on lap of) Joseph Sr., Rose (behind) Patricia, Kathleen, Joseph Jr. (behind) Rosemary. Dog in foreground is “Buddy.”
Though John F. Kennedy and Jackie might be the most recognizable members of the family, the Kennedys were famous long before John became president.
Their father, Joe Kennedy Sr., was a prominent businessman in Boston and his wife, Rose, was a noted philanthropist and socialite. Together they had nine children, three of whom went into politics. For the most part they lived their lives in the open, almost like America’s version of a royal family.
But, like every family, they had their secrets.
Born in 1918, Rosemary Kennedy was the third child of Joe and Rose and the first girl. During her birth, the obstetrician who was supposed to be delivering her was running late. Not wanting to deliver the baby without a doctor present, the nurse reached up into Rose’s birth canal and held the baby in place.
The actions of the nurse would have lasting consequences for Rosemary Kennedy. The lack of oxygen delivered to her brain during her birth caused lasting damage to her brain, resulting in a mental deficiency.
Though she looked like the rest of the Kennedys, with bright eyes and dark hair, her parents knew she was different right away.
As a child, Rosemary was unable to keep up with her siblings, who would often play ball in the yard, or run around the neighborhood. Her lack of inclusion often caused “fits,” which were later discovered to be seizures or episodes relating to her mental illness.
However, in the 1920s mental illness was highly stigmatized. Fearing repercussions if her daughter couldn’t keep up, Rose pulled Rosemary out of school and instead hired a tutor to teach the girl from home. Eventually, she sent her to a boarding school, in lieu of institutionalizing her.
In 1928, Joe was named an ambassador to the Court of St. James in England. The entire family moved across the Atlantic and was presented at court to the public. Despite her disabilities, Rosemary joined the family for the presentation.
Of course, no one knew the extent of her disability, as the Kennedys had worked hard to keep it quiet.
Keystone/Getty Images Rosemary, her sister Kathleen, and her mother Rose being presented to the people in London. Her family abandoned her and kept her shuttered away in institutions for the rest of her life.
In England, Rosemary gained a sense of normalcy, as she had been placed in a Catholic school run by nuns. With the time and patience to teach her, they were training her to be a teacher’s aide and she was flourishing under their guidance.
However, in 1940, when Germany marched on Paris, the Kennedys were forced back to the states, and Rosemary’s education was abandoned. Once back stateside, Rose placed Rosemary in a convent, though it didn’t last long. According to the nuns, Rosemary would sneak out at night and go to bars, meet strange men and go home with them.
At the same time, Joe was grooming his two oldest boys for a career in politics. Rose and Joe worried that Rosemary’s behavior could create a bad reputation not just for herself but for the whole family, and eagerly searched for something that would help her.
Dr. Walter Freeman was the answer.
Freeman, along with his associate Dr. James Watts had been researching a neurological procedure that was said to cure the physically and mentally disabled. The procedure? The lobotomy.
When it was first introduced, the lobotomy was hailed as a cure-all and was widely recommended by physicians. Despite the excitement, however, there were many warnings that the lobotomy, though occasionally effective, was also destructive. One woman described her daughter, a recipient, as being the same person on the outside, but like a new human on the inside.
John F. Kennedy Presidential Library and Museum The Kennedy family, not including baby Jean.
Despite the warnings, Joe needed no convincing, as it seemed like this was the Kennedy family’s last hope. Years later, Rose would claim that she had no knowledge of the procedure until it had already happened. No one thought to ask if Rosemary had any thoughts of her own.
In 1941, when she was 23 years old, Rosemary Kennedy received a lobotomy. Two holes were drilled in her skull, through which small metal spatulas were inserted. The spatulas were used to sever the link between the pre-frontal cortex and the rest of the brain. Though it is not known whether he did so on Rosemary, Dr. Freeman would often insert an icepick through the patient’s eye to sever the link as well as the spatula.
Throughout the entire procedure, Rosemary was awake, speaking with doctors and reciting poems to nurses. They knew the procedure was over when she stopped speaking.
Immediately after the procedure, the Kennedys realized that something was wrong.
John F. Kennedy Presidential Library and Museum John and his siblings Eunice, Joseph Jr., Rosemary, and Kathleen in a boat at Cohasset, Massachusetts, circa 1923-1924.
Rosemary could no longer speak or walk. She was moved to an institution and spent months in physical therapy before she regained movement, and even then it was only partially in one arm.
Rosemary Kennedy spent 20 years in the institution, unable to speak, walk, or see her family. It wasn’t until after Joe suffered a massive stroke that Rose went to go see her daughter again. In a panicked rage, Rosemary attacked her mother, unable to express herself any other way.
At that point, the Kennedys realized what they had done and began to champion rights for the mentally disabled.
John F. Kennedy would use his presidency to sign the Maternal and Child Health and Mental Retardation Planning Amendment to the Social Security Act, the precursor to the Americans with Disabilities Act, which his brother Ted pushed for during his time as a senator. Eunice Kennedy, JFK and Rosemary’s sister also founded the Special Olympics in 1962, to champion the achievements and abilities of the physically and mentally disabled.
After being reunited with her family, Rosemary Kennedy lived out the rest of her life in Saint Coletta’s, a residential care facility in Jefferson, Wisconsin, until her death in 2005.
The Bhavachakra is a Tibetan Buddhist representation of the “wheel of life,” or cycle of existence. MarenYumi/Flickr
The rich iconography of the Wheel of Life can be interpreted on several levels. The six major sections represent the Six Realms. These realms can be understood as forms of existence, or states of mind, into which beings are born according to their karma. The realms also can be viewed as situations in life or even personality types—hungry ghosts are addicts; devas are privileged; hell beings have anger issues.
In each of the realms, the Bodhisattva Avalokiteshvara appears to show the way to liberation from the Wheel. But liberation is possible only in the human realm. From there, those who realize enlightenment find their way out of the Wheel to Nirvana.
The gallery shows sections of the Wheel and explains them in more detail.
The Wheel of Life is one of the most common subjects of Buddhist art. The detailed symbolism of the Wheel can be interpreted on many levels.
The Wheel of Life (called the Bhavachakra in Sanskrit) represents the cycle of birth and rebirth and existence in samsara.
This gallery looks at different parts of the Wheel and explains what they mean. The main sections are the hub and the six “pie wedges” depicting the Six Realms. The gallery also looks at the Buddha figures in the corners and at Yama, the fearsome creature holding the Wheel in his hooves.
Many Buddhists understand the Wheel in an allegorical, not literal, way. As you examine the parts of the wheel you might find yourself relating to some of it personally or recognizing people you know as Jealous Gods or Hell Beings or Hungry Ghosts.
The outer circle of the Wheel (not shown in detail in this gallery) is the Paticca Samuppada, the Links of Dependent Origination. Traditionally, the outer wheel depicts a blind man or woman (representing ignorance); potters (formation); a monkey (consciousness); two men in a boat (mind and body); a house with six windows (the senses); an embracing couple (contact); an eye pierced by an arrow (sensation); a person drinking (thirst); a man gathering fruit (grasping); a couple making love (becoming); a woman giving birth (birth); and a man carrying a corpse (death).
Yama, Lord of the Underworld
The Wrathful Dharmapala of Hell Yama, Lord of the Underworld, represents death and holds the wheel in his hooves. MarenYumi/Flickr
The creature holding the Wheel of Life in his hooves is Yama, the wrathful dharmapala who is Lord of the Hell Realm.
The terrible face of Yama, who represents impermanence, peers over the top of the Wheel. In spite of his appearance, Yama is not evil. He is a wrathful dharmapala, a creature devoted to protecting Buddhism and Buddhists. Although we may be frightened of death, it is not evil; just inevitable.
In legend, Yama was a holy man who believed he would realize enlightenment if he meditated in a cave for 50 years. In the 11th month of the 49th year, robbers entered the cave with a stolen bull and cut off the bull’s head. When they realized the holy man had seen them, the robbers cut off his head also.
But the holy man put on the bull’s head and assumed the terrible form of Yama. He killed the robbers, drank their blood, and threatened all of Tibet. He could not be stopped until Manjushri, Bodhisattva of Wisdom, manifested as the even more terrible dharmapala Yamantaka and defeated Yama. Yama then became a protector of Buddhism.
The Realm of the Gods
Being a God Isn’t Perfect The Realm of the Gods of the Bhavachakra. MarenYumi/Flickr
The Realm of the Gods (Devas) is the highest realm of the Wheel of Life and is always depicted at the top of the Wheel.
The Realm of the Gods (Devas) sounds like a nice place to live. And, no question, you can do a lot worse. But even the Realm of the Gods isn’t perfect. Those born in the God Realm live long and pleasure-filled lives. They have wealth and power and happiness. So what’s the catch?
The catch is that because the Devas have such rich and happy lives they don’t recognize the truth of suffering. Their happiness is, in a way, a curse, because they have no motivation to seek liberation from the Wheel. Eventually, their happy lives end, and they must face rebirth in another, less happy, realm.
The Devas are perpetually at war with their neighbors on the Wheel, the Asuras. This depiction of the Wheel shows the Devas charging the Asuras.
The Realm of Asuras
Jealous Gods and Paranoia The Realm of Asuras, also called Jealous Gods or Titans. MarenYumi/Flickr
The Asura (Jealous God) Realm is marked by paranoia.
Asuras are hyper-competitive and paranoid. They are driven by a desire to beat their competition, and everyone is competition. They have power and resources and sometimes accomplish good things with them. But, always, their first priority is getting to the top. I think of powerful politicians or corporate leaders when I think of Asuras.
Chih-i (538-597), a patriarch of the T’ien-t’ai school, described the Asura this way: “Always desiring to be superior to others, having no patience for inferiors and belittling strangers; like a hawk, flying high above and looking down on others, and yet outwardly displaying justice, worship, wisdom, and faith — this is raising up the lowest order of good and walking the way of the Asuras.”
Asuras, who are also called “anti-gods,” are perpetually at war with the Devas of the God Realm. Asuras think they belong in the God Realm and fight to get in, although here it seems the Asuras have formed a line of defense and are fighting the attacking Devas with bows and arrows. Some depictions of the Wheel of Life combine the Asura and God realms into one.
Sometimes there is a beautiful tree growing between the two realms, with its roots and trunk in the Asura Realm. But its branches and fruit are in the God Realm.
The Realm of Hungry Ghosts
Craving That Can Never Be Satisfied The Realm of Hungry Ghosts. MarenYumi/Flickr
Hungry Ghosts have huge, empty stomachs, but their thin necks don’t allow nourishment to pass. Food turns to fire and ash in their mouths.
Hungry Ghosts (Pretas) are pitable things. They are wasted creatures with huge, empty stomachs. Their necks are too thin to allow food to pass. So, they are constantly hungry.
Greed and jealousy lead to rebirth as a Hungry Ghost. The Hungry Ghost Realm often, but not always, is depicted between the Asura Realm and the Hell Realm. It is thought the karma of their lives was not quite bad enough for a rebirth in the Hell Realm but not good enough for the Asura Realm.
Psychologically, Hungry Ghosts are associated with addictions, compulsions and obsessions. People who have everything but always want more may be Hungry Ghosts.
The Hell Realm
Fire and Ice The Hell Realm of the Wheel of Life. MarenYumi/Flickr
The Hell Realm is marked by anger, terror and claustrophobia.
The Hell Realm is depicted as a place partly of fire and partly of ice. In the fiery part of the realm, Hell Beings (Narakas) are subjected to pain and torment. In the icy part, they are frozen.
Interpreted psychologically, Hell Beings are recognized by their acute aggression. Fiery Hell Beings are angry and abusive, and they drive away anyone who would befriend or love them. Icy Hell Beings shove others away with their unfeeling coldness. Then, in the torment of their isolation, their aggression increasingly turns inward, and they become self-destructive.
The Animal Realm
No Sense of Humor The Animal Realm of the Wheel of Life. MarenYumi/Flickr
Animal Beings (Tiryakas) are solid, regular and predictable. They cling to what is familiar and are disinterested, even fearful, of anything unfamiliar.
The Animal Realm is marked by ignorance and complacency. Animal Beings are stolidly un-curious and are repelled by anything unfamiliar. They go through life seeking comfort and avoiding discomfort. They have no sense of humor.
Animal Beings may find contentment, but they easily become fearful when placed in a new situation. Naturally, they are bigoted and likely to remain so. At the same time, they are subject to oppression by other beings — animals do devour each other, you know.
The Human Realm
The Hope of Liberation The human realm of the Wheel of Life. MarenYumi/Flickr
Liberation from the Wheel is possible only from the Human Realm.
The Human Realm is marked by questioning and curiosity. It is also a realm of passion; human beings (Manushyas) want to strive, consume, acquire, enjoy, explore. Here the Dharma is openly available, yet only a few seek it. The rest become caught up in striving, consuming and acquiring, and miss the opportunity.
The Center
What Makes the Wheel Turn The center of the Wheel of Life. MarenYumi/Flickr
At the center of the Wheel of Life are the forces that keep it turning — greed, anger and ignorance.
At the center of every Wheel of Life are a cock, a snake and a pig, which represent greed, anger and ignorance. In Buddhism, greed, anger (or hate) and ignorance are called the “Three Poisons” because they poison whoever harbors them. These are the forces that keep the Wheel of Life turning, according to the Buddha’s teaching of the Second Noble Truth.
The circle outside the center, which is sometimes missing in depictions of the Wheel, is called the Sidpa Bardo, or intermediate state. It is also sometimes called the White Path and the Dark Path. On one side, bodhisattvas guide beings to rebirths in the higher realms of Devas, Gods and Humans. On the other, demons lead beings to the lower realms of Hungry Ghosts, Hell Beings and Animals.
The Buddha
The Dharmakaya Buddha The Buddha. MarenYumi/Flickr
In the upper right-hand corner of the Wheel of Life, the Buddha appears, representing hope for liberation.
In many depictions of the Wheel of Life, the figure in the upper right-hand corner is a Dharmakaya Buddha. The dharmakaya is sometimes called the Truth Body or the Dharma Body and is identified with shunyata. Dharmakaya is everything, unmanifested, free of characteristics and distinctions.
Often this Buddha is shown pointing to the moon, which represents enlightenment. However, in this version the Buddha stands with his hands raised, as if in blessing.
The Door to Nirvana
The upper left-hand corner of a Bhavachakra is filled with a scene or symbol representing liberation from the Wheel. MarenYumi/Flickr
This depiction of the Wheel of Life shows the entry to Nirvana in the upper left-hand corner.
In the upper left-hand corner of this depiction of the Wheel of Life is a temple with a seated Buddha. A stream of beings rise from the Human Realms toward the temple, which represents Nirvana. Artists creating a Wheel of Life fill this corner in various ways. Sometimes the upper left-hand figure is a Nirmanakaya Buddha, representing bliss. Sometimes the artist paints a moon, which symbolizes liberation.
Reference
O’Brien, Barbara. “The Wheel of Life.” Learn Religions, Feb. 11, 2020, learnreligions.com/the-wheel-of-life-4123213.
The Student Homophile League, the first gay student organization in the country, was founded at Columbia University in 1966 and held many of its activities in Earl Hall.
In 1970, the group became the more activist Gay People at Columbia (also known as Gay People at Columbia-Barnard), which sponsored a series of popular Friday-night dances in Earl Hall’s auditorium.
In 1971, gay students established a gay lounge in Furnald Hall, which is now known as the Stephen Donaldson Queer Lounge.
Credit: Christopher D. Brazee/NYC LGBT Historic Sites Project, 2016.
HISTORY
In 1966, Columbia University became the first collegiate institution in the United States, and possibly the first in the world, with an LGBT student group. In the fall of that year, bisexual sophomore Robert Martin (using the pseudonym Stephen Donaldson) founded the Student Homophile League (SHL) following a meeting with Columbia and Barnard representatives, religious advisers, and two of the most important national leaders for gay and lesbian rights, Frank Kameny and Barbara Gittings.
The small student group had the support of the university chaplain and, thus, gained space in Earl Hall, the center of student religious life. The university officially recognized the group in April 1967 with the stipulation that it not organize social events. A subsequent front page article in the New York Times resulted in outrage from hundreds of alumni and negative editorials in many newspapers; one alum wrote “Tolerance has its limits. Let the pansies go elsewhere.” The SHL sponsored lectures, held “rap sessions” about homosexuality on dorm floors, and advocated for the acceptance of homosexuals in society in generally, with specific emphasis on ending discrimination in the military and the psychiatric community.
By 1970, Columbia’s gay student group had become the more activist Gay People at Columbia (also known as Gay People at Columbia-Barnard), which sought to “present as complete a view as possible of the contemporary gay experience: socially, educationally and politically.” Its most popular activity was monthly Friday-night dances, beginning in 1970, held in the auditorium on the third floor of Earl Hall, which welcomed the entire gay and lesbian community of New York. The dances reached their peak popularity in the 1980s and were especially popular with those who enjoyed the relaxed atmosphere that contrasted with the clubs and bars downtown. The group still exists as the Columbia Queer Alliance (CQA) and hosts “First Friday” dance events in Alfred Lerner Hall.
In 1971, gay students, led by Morty Manford (later the head of the Gay Activists Alliance and son of PFLAG founder Jeanne Manford), requested space for a gay lounge. Although denied permission by the university, the group took over an unused space in the basement of the Furnald Hall dormitory. The lounge eventually was recognized by the university and the space is still in use, now known as the Stephen Donaldson Queer Lounge.
In March 2018, the NYC LGBT Historic Sites Project successfully nominated Earl Hall to the National Register of Historic Places, following its listing on the New York State Register in January 2018. The nomination is available in the “Read More” section below.
Reference
Student Homophile League at Earl Hall, Columbia University ,Student Homophile League at Earl Hall, Columbia University,
I learned what “racial play” is and had a rather shitty experience with a “straight” guy who was into having sex with men.
ILLUSTRATIONS BY CLAIRE MILBRATH
After breaking up with a boyfriend in 2011, I wanted to explore online dating and give being single in Toronto a shot before jumping into anything serious. Unfortunately for me, I soon realized that the gay dating world came with its own set of rules, most of which are pretty weird and somewhat racist. Race, body shaming, identity politics, and masculinity seemed to come up a lot and eventually I just said “fuck it” and deleted every dating site I was on. I needed a break. I needed to hear something other than “looking for whites only” or “straight-acting only.” It got to a point where I felt shitty about wanting to get laid and needed give the online thing a rest.
In 2013, I came out of “online dating retirement” and decided to explore it again. Every so often I’d hear my friends gush about all the great dates and hot sex they were having on Grindr and Scruff. It took a lot of convincing, but I gave a few of these apps a shot. I downloaded both Grindr and Scruff and immediately starting messaging people.
Throughout that year, there were a few really nice conversations that didn’t really go anywhere, the occasional good ass and/or dick pics, and an older couple in their 80s that always messaged me in Spanish. But aside from that, the string of weird encounters just got worse every time. In January, I finally deleted all the apps and have sworn off online dating and hookups for good. But it wasn’t all for nothing. Below, you’ll find three stories that I’ll probably never forget.
Picture Tag Gone Wrong
Around Thanksgiving last year, I got a message from an Irish guy visiting the city for a few weeks. I chatted him up about all things Ireland and told him about a trip I was planning for spring 2016. The vibe was friendly for the first few days, and then he wanted to see some pics, which I was more than willing to share. I sent a face pic to start and he sent one back. He was a bald, rugged, bearded man with green eyes. Suffice to say the dude was really hot and definitely checked off a few boxes in the “my type” department.
We talked for a week and he eventually asked me if I had a dick pic. I sent the most recent one and waited for him to send something back. Two hours later he sends a pic, but it’s not of a body part or another sexy face pic, it’s a picture of him and his sister with the caption “hot pic.” I wasn’t sure if this was a mistake or a joke, but I decided to just brush it off and send another dick pic. He then responded with a picture of him smiling with his grandmother, saying nothing else.
Two days later he messaged me to ask what I was doing. I told him I was just enjoying my day off and asked him what he had planned for the day. He then sent a picture of his spread asshole dripping with cum, a picture of him and his dog, and then a picture of him having family dinner, again saying nothing else. At this point, I wasn’t even mad or upset. The dude clearly wasn’t serious. That or he had a fucked-up sense of humor.
As funny as the whole thing was, I decided to stop communicating with him entirely. I often wonder what a dripping asshole, playing with your dog, and eating dinner with your family could be code for, but I guess I’ll ever know.
“Racial Play” I messaged a guy after work one day just to see if he’d reply. He messaged me back and said he comes to Toronto for work every day and wondered if we could hook up later that evening. I told him we should drink a few beers at my place and see where it goes. He came over around 10:30 PM, and made a few weird comments about the beer we were drinking, calling it “hipster beer.” That sort of turned me off, but I decided not to read too much into it.
I wasn’t expecting things to heat up after the weird beer comment, but after six beers we just went for it and started making out. Before things escalated, he stopped me and said he needed to tell me something. I remember being puzzled and asking what was wrong. He told me he was into a few kinks, but didn’t know how to talk about them. Fetish is always an awkward subject for people, but I assured him I wasn’t easily weirded out. He looked extremely flustered and scared to say it, but after about five minutes of circling around the big confession, he sheepishly blurted out that he was into “racial play.”
I kind of giggled and then looked at him again. At that moment I realized he was being serious and took a deep breath because, as a black man and a human being, the whole thing had just thrown me off. Solely based on curiosity, I asked him exactly what this type of roleplay scene would entail. It scared me to imagine where this conversation was going to go, but I still couldn’t quite process what I just heard. I’ve done some weird shit, but this whole thing was fucked up and I didn’t understand what turned him on about it exactly. He asked me if I was mad that he was into that. I told him no because I actually wasn’t pissed at all. After having another beer he got into the finer details of how a “racial play” scene would go down.
According to him, a play scene would involve me in a cage, getting choked with his dick, while he spits on me and calls me nigger a few times. He assured me that while it was a lot to handle, it was actually a pretty popular fetish. It’s just something that nobody talks about. I looked at him, extremely puzzled after that statement. He stood, confident in his belief that was an acceptable thing to get off to, and it took a minute for me to figure out the best way to respond. Wanting to end this interaction on a peaceful note, I told him that while I respect his honesty, the thought of a man getting off to calling me racial slurs and performing violent sex acts on me was enough to make me want to commit murder.
When I said that he laughed it off, but once he saw the expression on my face, I could tell he knew it was probably in his best interest to call it a night. After he left I Googled “racial play” and found a lot of crazy shit, most of which I wish I could unsee. There are certain thoughts and images that linger in the subconscious and lead us to the fetishes we have. I think most things are fair game, but if me picking cotton gets you horny, there probably won’t be a second date.
Runaway Cucumber One of the first guys I met on Grindr was a university student who had just moved to Toronto for school. During our first hangout we drank a few beers and talked about Toronto, which was a nice change from the usual in-and-out hook up. We immediately hit it off and it turned into an ongoing thing. We met up for sex about twice a month for a couple of months. It was really low-key, which has awesome because I wasn’t after anything serious at the time.
One night he came over and dropped a bomb on me. Apparently he had a girlfriend, which was news to me. He said he wasn’t gay—he just met up with guys because his girlfriend wasn’t into anal play. This all seemed messy and complicated, so I told him we should cool it on the sex until he and his girlfriend had a serious conversation. It would be one thing if they were in an open relationship, but it seemed more like their lack of communication had led to him sneaking out to get fucked by guys behind her back. It just didn’t seem healthy for me to continue sleeping with him if that was the case.
He texted me out of the blue three months later, asking if we could meet. I had my reservations about it, but I decided to let him stop by and get an update on what was going on with him and his situation. He came over and immediately went for my crotch, but before I could let it go any further, I needed to ask what the status of his relationship was. Apparently he had broken up with his girlfriend and was exclusively fucking guys. The way he talked about these new relationships was very strange. He maintained that he was still straight, but just really loved bottoming and couldn’t get enough.
We proceeded to play around a bit and eventually I was fucking him. I don’t know if fate was punishing me for allowing my thirst to blind me from the obvious mess of a situation this was, but ten minutes into it I’d felt something wet go down my leg. Let’s just say that he wasn’t ready to bottom and by the time I stopped the evidence of that was all over my bed.
When you’re having butt sex, there’s always the slight possibility of a little shit, but this was literally a shit storm. He felt really bad and I didn’t want to make a big deal about it, so I said we should just shower and call it a night. I let him go first so I could throw away the sheets and after he got out I went in to get myself cleaned up. When I walked out of the shower, what I saw him doing brought new meaning to the phrase “by any means necessary.” I stood quietly by the door and watched as he began squatting down on a cucumber from my fridge, trying to fuck himself with it. He was jerking off and heavily breathing as he attempted to fit the entire cucumber up his ass.
After a minute or so, I purposely slammed the bathroom door and he freaked out when he saw me standing there. He could tell I was pissed and he kept trying to avoid eye contact. I asked him what he was doing still naked, which left him stuttering as he tried to make up a good excuse. I snatched the cucumber out of his hand and asked him to put on his clothes while I finished getting dressed in the bathroom.
After we were both dressed I walked him out of my apartment and told him he shouldn’t contact me again. I didn’t want to be an asshole, but between his first lie about the girlfriend and the shit-stained bed I had to throw out, I felt like the universe was trying to tell me this needed to end.
To make matters worse, when I went back into the house, I checked the fridge and the fucking cucumber was gone. I was short an ingredient for my next lunch. I ordered a new bed and went to buy groceries the next day. Thank you universe! I definitely got the message.
As you seem to have noticed, in the “Humpty Dumpty” nursery rhyme, nowhere does it say that Humpty is an egg, yet he is often presented as such in pictures and stories. The version of the rhyme that most children learn today goes like this:
Humpty Dumpty sat on a wall, Humpty Dumpty had a great fall.
All the king’s horses and all the king’s men Couldn’t put Humpty together again
The first known publication of Humpty Dumpty was included in Juvenile Amusements by Samuel Arnold in 1797. In that version, the last lines read “Fourscore men and fourscore more / could not make Humpty Dumpty where he was before.” Over the next century, the rhyme appeared in numerous books with variations on the lyrics.
These publications did not include the first use of the term “humpty dumpty,” though. According to the Oxford English Dictionary, “humpty dumpty” was first used in the 17th century and referred to brandy boiled with ale. In the 1700s, it was also a term used to describe a short, clumsy person. It has also been a nickname attributed to someone who has had too much alcohol (perhaps imbibing the drink of the same name).
As the popular nursery rhyme is neither a bottle of alcohol nor a person, it is most likely that the nursery rhyme was intended as a riddle. The answer to the riddle, of course, is “an egg”—something that, if it rolled off a wall, could not be mended by any number of people. Today, the answer is so well known that the character of Humpty Dumpty has taken on the appearance of an egg and the rhyme is not considered to be a riddle at all, but a story.
Because of this switch from “riddle” to “story”, many people today believe that there is more meaning to the nursery rhyme than is given in the lyrics. Perhaps, in this instance, we could take advice from Humpty Dumpty himself, as seen in Through the Looking Glass by Lewis Carroll: “When I use a word, it means just what I choose it to mean—neither more nor less.” People will always attribute more meaning to nursery rhymes than was initially intended.
Nursery rhymes are commonly linked to historical events, but it is difficult to prove that imagery in the nursery rhymes represents historical places and figures. Most modern rhymes, after all, are created with the intent of being silly, repetitive, and enjoyable for children to repeat rather than for their historical significance (think “Miss Mary Mack” and other clapping games).
Two of the most popular theories link Humpty Dumpty to two separate historical events. The first is the Fall of Colchester. During the English Civil War in 1648, the town of Colchester was under siege. Supposedly, a man named Jack Thompson was stationed on the walls with a cannon nicknamed “Humpty Dumpty.” Thompson and the cannon managed to do a lot of damage to the advancing Parliamentarian troops, until the cannon eventually tumbled to the ground. Given the size and weight of the cannon, the dozens of men who attempted to lift it back to its place on the wall were unable to do so. Eventually, Colchester was forced to open its gates and surrender. While the siege of Colchester did happen, it is unlikely that Humpty Dumpty refers to anything in the siege as it happened over a century before Humpty Dumpty was recorded and there is no documented connection between the two.
The other popular theory is that Humpty Dumpty represented King Richard III. , called the “humpbacked king”. (He supposedly was a hunchback, though recent evidence seems to indicate Shakespeare was wildly exaggerating on this point, with Richard actually apparently having scoliosis which made his right shoulder higher than the left, but otherwise no hunch). In 1485, Richard III fought at the Battle of Bosworth. In this “humpty dumpty” origin story, it was said that either his horse was named “Wall” or his men, who abandoned him, were representative of the “wall.” Either way, the king fell off his horse and was supposedly hacked to pieces on the field—thus no one could put him together again. Several problems exist with this theory, the least of which being that the term “humpbacked” didn’t exist in King Richard’s day, nor for several centuries after. (The term “hunchback” also didn’t first pop up until the 18th century). Much more importantly was that the king’s remains were recently found largely intact save for a bludgeon to the head which probably killed him. Additionally, other than pure speculation, as in the previous “siege of Colchester” theory, no solid historical evidence has been found that shows that King Richard III was the inspiration for Humpty Dumpty. And, indeed, one of the reasons it’s so often connected, because of the “all the king’s horses and all the king’s men” bit, as noted, wasn’t even in the original version, being the more generic “fourscore men and fourscore more”.
The historical events that have been linked to “Humpty Dumpty” provide excellent stories, but are based on pure speculation. Given the actual evidence at hand, it is far more likely that Humpty Dumpty was not intended to be a story, but rather just a riddle posed to children for their amusement. The answer to the riddle, as stated, is “an egg”, which is why Humpty Dumpty today is nearly always depicted as such.
The Five Dhyani Buddhas are icons of Mahayana Buddhism. These transcendent Buddhas are visualized in tantric meditation and appear in Buddhist iconography.
The five Buddhas are Aksobhya, Amitabha, Amoghasiddhi, Ratnasaṃbhava, and Vairocana. Each represents a different aspect of enlightened consciousness to aid in spiritual transformation.
Often in Vajrayana art, they are arranged in a mandala, with Vairocana in the center. The other Buddhas are depicted in each of the four directions (north, south, east, and west).
Each Dhyani Buddha has a specific color and symbol which represent his meanings and the purpose for meditating on him. Mudras, or hand gestures, are also used in Buddhist art to distinguish one Buddha from another and convey the appropriate teaching.
Akshobhya was a monk who vowed never to feel anger or disgust toward another being. He was immovable in keeping this vow. After striving for a long period, he became a Buddha.
Akshobhya is a heavenly Buddha who reigns over the Eastern paradise, Abhirati. Those who fulfill Akshobhya’s vow are reborn in Abhirati and cannot fall back into lower states of consciousness.
It’s important to note that the directional ‘paradises’ are understood to be a state of mind, not physical places.
Depictions of Akshobhya
In Buddhist iconography, Akshobhya is usually blue though sometimes gold. He is most often pictured touching the earth with his right hand. This is the earth-touching mudra, which is the gesture used by the historical Buddha when he asked the earth to bear witness to his enlightenment.
In his left hand, Akshobhya holds a vajra, the symbol of shunyata — an absolute reality that is all things and beings, unmanifested. Akshobhya is also associated with the fifth skandha, consciousness.
In Buddhist tantra, evoking Akshobhya in meditation helps overcome anger and hatred.
Amitabha Buddha, who is also called Amita or Amida Buddha, is probably the best known of the Dhyani Buddhas. In particular, devotion to Amitabha is at the center of Pure Land Buddhism, one of the largest schools of Mahayana Buddhism in Asia.
In a long-ago time, Amitabha was a king who renounced his kingdom to become a monk. Called Dharmakara Bodhisattva, the monk practiced diligently for five eons and realized enlightenment and became a buddha.
Amitabha Buddha reigns over Sukhavati (the Western paradise) which is also called the Pure Land. Those reborn in the Pure Land experience the joy of hearing Amitabha teach the dharma until they are ready to enter Nirvana.
Depictions of Amitabha
Amitabha symbolizes mercy and wisdom. He is associated with the third skandha, that of perception. Tantric meditation on Amitabha is an antidote to desire. He is sometimes pictured in between the bodhisattvas Avalokiteshvara and Mahasthamaprapta.
In Buddhist iconography, Amitabha’s hands are most often in a meditation mudra: fingers barely touching and gently folded over the lap with palms facing upward. His red color symbolizes love and compassion and his symbol is the lotus, representing gentleness and purity.
In the “Bardo Thodol” — the “Tibetan Book of the Dead” — Amoghasiddhi Buddha appears to represent the accomplishment of all action. His name means ‘Infalliable Success” and his consort is the well-known Green Tara, in the ‘Noble Deliverer.’
Amoghasiddhi Buddha reigns in the North and is associated with the fourth skandha, volition or mental formations. This can also be interpreted as impulses, which is strongly associated with action. Meditation on Amoghasiddhi Buddha vanquishes envy and jealousy, two often impulsive actions.
Depictions of Amoghasiddhi
Amoghasiddhi is most often depicted in Buddhist iconography as radiating a green light, which is the light of accomplishing wisdom and promoting peace. His hand gesture is the mudra of fearlessness: his right hand in front of his chest and palm facing outward as if to say ‘stop.’
He holds a crossed vajra, also called a double dorje or the thunderbolt. This represents accomplishment and fulfillment in all directions.
Ratnasambhava Buddha represents richness. His name translates to “Origin of Jewel” or the “Jewel-Born One.” In Buddhism, the Three Jewels are the Buddha, the Dharma, and the Sangha and Ratnasambhava is often thought of as the giving Buddha.
He reigns in the South and is associated with the second skandha, sensation. Meditation on Ratnasambhava Buddha vanquishes pride and greed, focusing instead on equality.
Depictions of Ratnasambhava
Ratnasambhava Buddha has a yellow color which symbolizes earth and fertility in Buddhist iconography. He often holds a wish-fulfilling jewel.
He holds his hands in the wish-fulfilling mudra: his right hand facing down and the palm outward and his left in the mudra of meditation. This symbolizes generosity.
Vairocana Buddha is sometimes called the primordial Buddha or Supreme Buddha. He is thought to be the embodiment of all the Dhyani Buddhas; also everything and everywhere, omnipresent and omniscient.
He represents the wisdom of shunyata, or emptiness. Vairocana is considered a personification of the dharmakaya — everything, unmanifested, free of characteristics and distinctions.
He is associated with the first skandha, form. Meditation on Vairocana vanquishes ignorance and delusion, leading to wisdom.
Depictions of Vairocana
When the Dhyani Buddhas are pictured together in a mandala, Vairocana is at the center.
Vairocana is white, representing all colors of light and all the Buddhas. His symbol is the Dharma wheel, which, at its most basic, represents the study of the dharma, practice through meditation, and moral discipline.
His hand gesture is known as the Dharmachakra mudra and is often reserved for the iconography of either Vairocana or the historical Buddha, Shakyamuni. The mudra represents the turning of the wheel and places the hands so that the thumbs and index fingers touch at the tips to form a wheel.
Reference
O’Brien, Barbara. “The Five Dhyani Buddhas.” Learn Religions, Jan. 29, 2020, learnreligions.com/the-five-dhyani-buddhas-4123189.