The Bible has been translated into far more languages than any other book. Yet, as Harry Freedman reveals, the history of Bible translations is not only contentious but bloody, with many who dared translate it being burned at the stake…
In 1427, Pope Martin ordered that John Wycliffe’s bones be exhumed from their grave, burned and cast into the river Swift. Wycliffe had been dead for 40 years, but his offence still rankled.
John Wycliffe (c1330–1384) was 14th-century England’s outstanding thinker. A theologian by profession, he was called in to advise parliament in its negotiations with Rome. This was a world in which the church was all-powerful, and the more contact Wycliffe had with Rome, the more indignant he became. The papacy, he believed, reeked of corruption and self-interest. He was determined to do something about it.
Wycliffe began publishing pamphlets arguing that, rather than pursuing wealth and power, the church should have the poor at heart. In one tract he described the Pope as “the anti-Christ, the proud, worldly priest of Rome, and the most cursed of clippers and cut-purses”.
In 1377 the Bishop of London demanded that Wycliffe appear before his court to explain the “wonderful things which had streamed forth from his mouth”. The hearing was a farce. It began with a violent row over whether or not Wycliffe should sit down. John of Gaunt, the king’s son and an ally of Wycliffe, insisted that the accused remain seated; the bishop demanded that he stand.
When the Pope heard of the fiasco he issued a papal bull [an official papal letter or document] in which he accused Wycliffe of “vomiting out of the filthy dungeon of his heart most wicked and damnable heresies”. Wycliffe was accused of heresy and put under house arrest and was later forced to retire from his position as Master of Balliol College, Oxford.
Wycliffe firmly believed that the Bible should be available to everybody. He saw literacy as the key to the emancipation of the poor. Although parts of the Bible had previously been rendered into English there was still no complete translation. Ordinary people, who neither spoke Latin nor were able to read, could only learn from the clergy. Much of what they thought they knew – ideas like the fires of hell and purgatory – were not even part of Scripture.
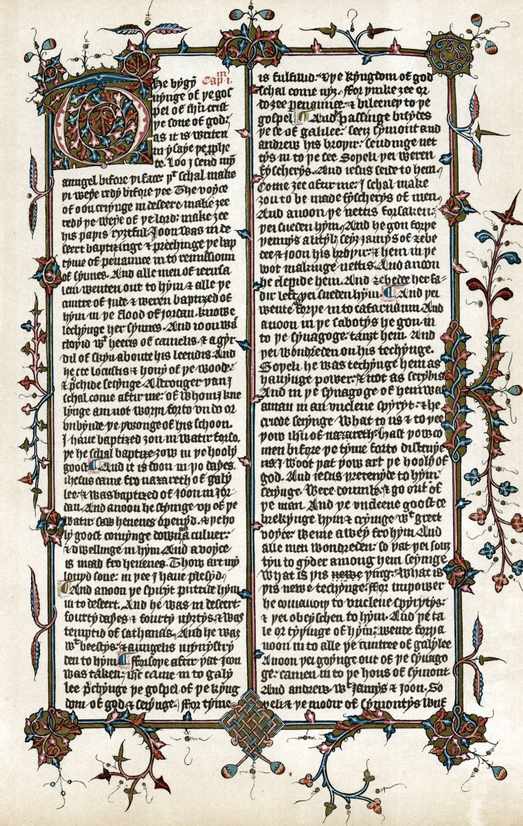
With the aid of his assistants, therefore, Wycliffe produced an English Bible [over a period of 13 years from 1382]. A backlash was inevitable: in 1391, before the Bible was completed, a bill was placed before parliament to outlaw the English Bible and to imprison anyone possessing a copy. The bill failed to pass – John of Gaunt saw to that [in parliament] – and the church resumed its persecution of the now-dead Wycliffe [he died in 1384].
Shorn of alternatives, the best they could do was to burn his bones [in 1427], just to make sure his resting place was not venerated. The Archbishop of Canterbury explained that Wycliffe had been “that pestilent wretch, of damnable memory, yea, the forerunner and disciple of antichrist who, as the complement of his wickedness, invented a new translation of the scriptures into his mother-tongue”.
A page from John Wycliffe’s translation of the Bible into English, c1400. (Photo by Ann Ronan Pictures/Print Collector/Getty Images)
Jan Hus
In 1402, the newly ordained Czech priest Jan Hus was appointed to a pulpit in Prague to minister in the church. Inspired by Wycliffe’s writings, which were now circulating in Europe, Hus used his pulpit to campaign for clerical reform and against church corruption.
Like Wycliffe, Hus believed that social reform could only be achieved through literacy. Giving the people a Bible written in the Czech language, instead of Latin, was an imperative. Hus assembled a team of scholars; in 1416 the first Czech Bible appeared. It was a direct challenge to those he called “the disciples of antichrist” and the consequence was predictable: Hus was arrested for heresy.
Jan Hus’s trial, which took place in the city of Constance, has gone down as one of the most spectacular in history. It was more like a carnival – nearly every bigwig in Europe was there. One archbishop arrived with 600 horses; 700 prostitutes offered their services; 500 people drowned in the lake; and the Pope fell off his carriage into a snowdrift. The atmosphere was so exhilarating that Hus’s eventual conviction and barbaric execution must have seemed an anti-climax. But slaughtered he was, burnt at the stake. His death galvanised his supporters into revolt. Priests and churches were attacked, the authorities retaliated. Within a few short years Bohemia had erupted into civil war. All because Jan Hus had the gall to translate the Bible.
The capture of Jan Hus. Miniature of the ‘Chronicle’ of Ulrich of Richental. Prague, national library of the University. (Photo by Roger Viollet Collection/Getty Images)
William Tyndale
As far as the English Bible is concerned, the most high profile translator to be murdered was William Tyndale. It was now the 16th century and Henry VIII was on the throne. Wycliffe’s translation was still banned, and although manuscript copies were available on the black market, they were hard to find and expensive to procure. Most people still had no inkling of what the Bible really said.
But printing was becoming commonplace, and Tyndale believed the time was right for an accessible, up-to-date translation. He knew he could create one; all he needed was the funding, and the blessing of the church. It didn’t take him long to realise that nobody in London was prepared to help him. Not even his friend, the bishop of London, Cuthbert Tunstall. Church politics made sure of that.
The religious climate appeared less oppressive in Germany. Luther had already translated the Bible into German; the Protestant Reformation was gathering pace and Tyndale believed he would have a better chance of realising his project there. So he travelled to Cologne and began printing.
This, it transpired, was a mistake. Cologne was still under the control of an archbishop loyal to Rome. He was halfway through printing the book of Matthew when he heard that the print shop was about to raided. He bundled up his papers and fled. It was a story that would be repeated several times over the next few years. Tyndale spent the next few years dodging English spies and Roman agents. But he managed to complete his Bible and copies were soon flooding into England – illegally, of course. The project was complete but Tyndale was a marked man.
He wasn’t the only one. In England, Cardinal Wolsey was conducting a campaign against Tyndale’s Bible. No one with a connection to Tyndale or his translation was safe. Thomas Hitton, a priest who had met Tyndale in Europe, confessed to smuggling two copies of the Bible into the country. He was charged with heresy and burnt alive.
Thomas Bilney, a lawyer whose connection to Tyndale was tangential at the most, was also thrown into the flames. First prosecuted by the bishop of London, Bilney recanted and was eventually released in 1529. But when he withdrew his recantation in 1531 he was re-arrested and prosecuted by Thomas Pelles, chancellor of Norwich diocese, and burnt by the secular authorities just outside the city of Norwich.
Meanwhile Richard Bayfield, a monk who had been one of Tyndale’s early supporters, was tortured incessantly before being tied to the stake. And a group of students in Oxford were left to rot in a dungeon that was used for storing salt fish.
Tyndale’s end was no less tragic. He was betrayed in 1535 by Henry Phillips, a dissolute young aristocrat who had stolen his [Phillips’] father’s money and gambled it away. Tyndale was hiding out in Antwerp, under the quasi–diplomatic protection of the English merchant community. Phillips, who was as charming as he was disreputable, befriended Tyndale and invited him out for dinner. As they left the English merchant house together, Phillips beckoned to a couple of thugs loitering in a doorway. They seized Tyndale. It was the last free moment of his life. Tyndale was charged with heresy in August 1536 and burnt at the stake a few weeks later.
William Tyndale being tied to a stake before being strangled and burned to death. (Photo by Hulton Archive/Getty Images)
England was not the only country to murder Bible translators. In Antwerp, the city where Tyndale thought he was safe, Jacob van Liesveldt produced a Dutch Bible. Like so many 16th-century translations, his act was political as well as religious. His Bible was illustrated with woodcuts – in the fifth edition he depicted Satan in the guise of a Catholic monk, with goat’s feet and a rosary. It was a step too far. Van Liesveldt was arrested, charged with heresy and put to death.
A murderous age
The 16th century was by far the most murderous age for Bible translators. But Bible translations have always generated strong emotions, and continue to do so even today. In 1960 the United States Air Force Reserve warned recruits against using the recently published Revised Standard Version because, they claimed, 30 people on its translation committee had been “affiliated with communist fronts”. TS Eliot, meanwhile, railed against the 1961 New English Bible, writing that it “astonishes in its combination of the vulgar, the trivial, and the pedantic”.
And Bible translators are still being murdered. Not necessarily for the act of translating the Bible, but because rendering the Bible into local dialects is one of the things Christian missionaries do. In 1993 Edmund Fabian was murdered in Papua New Guinea, killed by a local man who had been helping him translate the Bible. In March 2016, four Bible translators working for an American evangelical organisation were killed by militants in an undisclosed location in the Middle East.
Bible translations, then, may appear to be a harmless activity. History shows it is anything but.
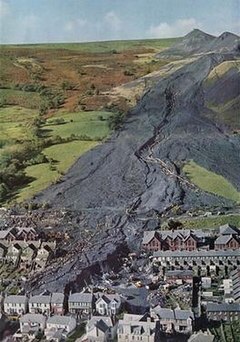
As the event that dominates the third episode of Season 3 of The Crown, the Aberfan Disaster remains one of the most devastating losses of human life in Welsh history. On the morning of October 21, 1966, the collapse of a soil tip triggered a slurry slide that ended 116 children and 28 adults in the village of Aberfan, Wales.
Located in Southern Wales, Aberfan was devastated by the disaster. Life revolved around nearby mining operations. As Aberfan residents carried out recovery and relief efforts, Queen Elizabeth II issued a statement – resisting the advice of Prime Minister Harold Wilson to visit the site of the tragedy.
The events leading up to and in the aftermath of the Aberfan Disaster ultimately changed the role of royalty, the lives of countless Welshmen and women, and mining safety in Britain.
The Mine Near Aberfan Was Under The Authority Of The National Coal Board Of Britain
The Merthyr Vale Colliery included seven tips, the first of which dated back to 1869. In 1966, the colliery encircled Arberfan, a village that served as home to miners and their families. The Merthyr Vale Colliery was regulated by the National Coal Board (NCB), the overseeing body that was formed in 1947. The NCB nationalized mining in the United Kingdom, promoting the industry and setting production and distribution guidelines.
When Tip 7 of the Merthyr Valley Colliery was begun in 1958, it was built over an underground spring, creating an intrinsic instability. There were several tips at the mine built over these springs, resulting in several slips during the 1960s. In 1963, for example, an engineer at the mine noted, “danger from coal slurry being tipped at the rear of Pantglas School,” but the NCB failed to act on the warning.
Aberfan Experienced Heavy Rains That Caused A Great Amount Of Ground Instability
October 1966 was a particularly rainy month for Aberfan and the surrounding region, with roughly 60 inches falling in the weeks preceding the disaster. As water filled streams and underground springs, the slag heap – where the mine discarded its waste – were susceptible to heavy rain, as well.
Tip 7 began to show signs of weakness during the early hours on October 21, 1966. At around 7:30 am, mine workers observed settlement at the tip, something that increased over the subsequent hours. First 10 feet, then 10 feet more – the top of the tip was slowly giving way. Reportedly, the crew took a break, intent on working to remedy the problem as soon as they were done.
A Collapse At Tip 7 Of The Mine Triggered A Slurry Surge That Struck A Nearby School
The students at Pantglas Junior School arrived for classes on Friday, October 21, 1966, expecting to enjoy the last day of school before their midterm break. The night before, 9-year-old Eryl Jones dreamed that school had been canceled for that day, describing “something black came down all over it” to her mother before she left home that morning.
When the school opened at 9 am, 240 students entered. However, within minutes, they heard what survivor Gaynor Madgewick described as:
A terrible, terrible sound, a rumbling sound. It was so loud. I just didn’t know what it was. It seemed like the school went numb, you could hear a pin drop. I was suddenly petrified and glued to the chair. It sounded like the end of the world had come.
What Madgewick heard was a flood of slurry – a mixture of water, mud, and coal debris – descending the mountain as it approached the school. Other survivors described the sound as akin to, “a jet plane screaming low over the school in the fog.”
As the slide began, one of the workers at Tip 7 observed, “It started to rise slowly at first, sir… I thought I was seeing things. Then it rose up pretty fast, sir, at a tremendous speed. Then it sort of came up out of the depression and turned itself into a wave… down towards the mountain… towards Aberfan village… into the mist.”
Children Later Recalled Struggling To Breathe While Buried Under Waste
When the slurry hit Pantglas Junior School, children and teachers alike were immediately buried under “a [slurry] wave over 12 meters high and 7 meters wide traveling at speed down the valley.”
There had been no warning since the telephone cables leading to the tip had been taken. As it approached the school, it wiped out the entire landscape, eventually leaving 6 to 9 meters of debris. Brian Williams, 7 years old at the time, “watched the classroom wall split from the bottom to the top. The wall came through and stopped. And the next thing I remember was it went very quiet, and then a lot of screaming and crying.” Williams had escaped being under the crumbling wall, having been shifted to another desk across the room moments before.
Survivor Jeff Edwards remembered “waking up [and] my right foot was stuck in the radiator and there was water pouring out of it. My desk was pinned against my stomach and a girl’s head was on my left shoulder. She was dead. Because all the debris was around me I couldn’t get away from her. The image of her face comes back to me continuously.”
Edwards spent the next 90 minutes listening to the “crying and screaming” of his classmates, but “as time went on they got quieter and quieter as children died, they were buried and running out of air.” He, too, struggled to breathe as he lay under the mixture of coal, water, and mud.
Residents And Professional Miners Alike Tried To Dig To Find Survivors
Miners, bystanders, and municipal authorities frantically rushed toward the school. When police officer Yvonne Price, 21 years old at the time, arrived, she “was rigid with shock… you could see doors, tables, kitchen utensils floating in” black water. She witnessed “people from the village passing saucepans and buckets full of debris.”
The New York Times later reported, “Civil defense teams, miners, policemen, firemen and other volunteers toiled desperately, sometimes tearing at the coal rubble with their bare hands, to extricate the children. Bulldozers shoved debris aside to get to the children. A hush fell on the rescuers once when faint cries were heard in the rubble.”
Due to her small size, Officer Price was sent through a hole in the ground to see if she could find any survivors. She found none.
Recovery efforts continued long after cries from under the debris could be heard. Alix Palmer, a journalist at Aberfan, saw, “the fathers straight from the pit… digging… no-one had yet really given up hope, although logic told them it was useless.” Every time a body was found, people would pause as a doctor made his way to check for signs of life. The last surviving child, Jeff Edwards, was pulled to safety at around 11 am.
Men and women continued to dig, pulling 67 bodies out of the rubble on the first day. One of the teachers, David Beynon, was discovered with five children in his arms. He had tried to protect them in their final moments. Nansi Williams, the school’s dinner lady, was collecting money when the slurry hit the school and she, too, lost her life protecting several students. All of the five children she covered with her body survived.
The Bodies Of Children Were Identified By Items They Had In Their Pockets
When Reverend Irving Penberthy arrived on the scene of the Aberfan Disaster, he “stayed with the people who were watching and waiting” before taking his post at the Bethania Chapel. Soon, the chapel became a mortuary, one that received the bodies of children as they were extracted from under the slurry. Penberthy recalled watching as “fathers – it was mainly fathers, of course, not the women – just going around and lifting the blanket, and then going on further, and the shock when they finally found their own child. That was dreadful. And all we did was just cry together.”
As more and more bodies arrived, Charles Nunn, assigned as the senior identification officer at Aberfan, wrote, “a description of each child or adult and detail any possessions in their pockets – a handkerchief, sweets, anything that might help with identification. The little ones were laid on the pews, the adults on stretchers across the tops of the pews – males to the left and females to the right. By about the fourth or fifth day we had to start taking bodies up a difficult winding staircase to the upstairs gallery.”
While many of the children perished as a result of asphyxiation; there were some bodies that were deemed unsuitable for viewing due to extensive injuries. In a letter to her mother, journalist Alix Palmer wrote, “the slag had had time to corrode the skin of the children still buried and many brought out burned could only been identified by the clothing or things in their pockets. One little boy… was identified by a slip of paper with his name on deep inside his wallet.”
The Queen Resisted Efforts To Get Her To Visit The Site
As details of the disaster emerged and bodies continued to be pulled from the debris (dozens on the first day alone), Queen Elizabeth II resisted pleas to visit Aberfan. Just as it was depicted in the third season of The Crown, the monarch opted to send a proxy – her husband, Prince Philip.
In her initial statement, she expressed sadness and sorrow. While the show indicated a lack of emotion on the part of the queen, it’s been asserted that she didn’t want to pull attention and resources away from rescue efforts. She was said to have insisted, “People will be looking after me… perhaps they’ll miss some poor child that might have been found in the wreckage.”
The British government was represented by Harold Wilson, the Prime Minister, and Lord Snowdon Antony Armstrong-Jones, Princess Margaret’s husband. The latter, according to Prime Minister Wilson, “made it his job to visit bereaved relatives… sitting holding the hands of a distraught father, sitting with the head of a mother on his shoulder for a half an hour in silence.”
Prince Philip spent two hours with relatives of victims, surveying the site, and visiting the cemetery where more than 81 children had already been laid to rest.
The Queen Did Make Her Way To Aberfan, Visiting The Day After The Last Body Was Recovered
Queen Elizabeth II arrived in Aberfan more than a week after the disaster struck and only one day after the last body was retrieved from the debris. When she and Prince Philip toured Aberfan on October 29, 1966, they were both visibly moved by the experience. As a young child handed Elizabeth a flower -“From the remaining children of Aberfan” – the stoic queen was said to have been on the brink of tears. According to Jeff Edwards, the last child to be found alive, “We know she did cry, because she went to Jim Williams’ house – and when she came down from the cemetery she was visibly crying.”
When the queen spoke to her subjects at Aberfan, she told them, “As a mother, I’m trying to understand what your feelings must be… I’m sorry I can give you nothing at present except sympathy.” The queen’s former private secretary, Lord Charteris, told author Gyles Brandreth that not going to Aberfan earlier was one of her biggest regrets.
Survivors see her visit differently, however. Edwards, again, noted, “When she did arrive she was visibly upset and the people of Aberfan appreciated her being here. She came when she could and nobody would condemn her for not coming earlier, especially as everything was such a mess.” Marjorie Collins, the mother of one of the victims, similarly saw the visit as a supportive endeavor, observing, “They [Prince Philip and Queen Elizabeth] were above the politics and the din and they proved to us that the world was with us, and that the world cared.”
The Disaster Could Have Been Prevented Had Earlier Concerns Been Addressed
In his comments about the disaster at Aberfan, the chairman of the National Coal Board (NCB), Lord Robens, noted the impossibility of knowing “that there was a spring in the heart of this tip [meaning Tip 7].”
The inquest and tribunal into the cause of the slide that took 144 lives thought otherwise, calling the event “a terrifying tale of bungling ineptitude by many men charged with tasks for which they were totally unfitted, of failure to heed clear warnings, and of a total lack of direction from above.”
The tribunal took place over 76 days, interviewing 136 witnesses and examining 300 exhibits. Earlier concerns about the tips were made very clear, as was the lack of NCB policy when it came to safely installing tips. In his testimony, Lord Robens ultimately admitted fault by the NCB, something with which the tribunal agreed, concluding in 1967:
Blame for the disaster rests upon the National Coal Board. This is shared, though in varying degrees, among the NCB headquarters, the South Western Divisional Board, and certain individuals… The legal liability of the NCB to pay compensation of the personal injuries, fatal or otherwise, and damage to property, is incontestable and uncontested.
No malice or criminality was found, but it was determined that the entire disaster could have been avoided but for “ignorance, ineptitude and a failure in communications.”
New Legislation Was Introduced In 1969 To Tighten The Oversight Of Mines
Mining regulations became increasingly stringent in the years after Aberfan. New legislation was, according to Prime Minister Harold Wilson in 1967, “desirable” in light of the recommendations made by the tribunal. When Wilson saw the findings of the Aberfan tribunal, he was shocked and deeply concerned by its “devastating nature.”
In 1969, two years after the tribunal’s findings, Lord Robens headed efforts that resulted in the 1974 Health and Safety at Work Act, legislation that continues to regulate mining in the United Kingdom. Although Robens had offered his resignation to the NCB, it was dismissed by members of Parliament and Prime Minister Harold Wilson – something that only contributed to Robens’s villainy in the eyes of the victims of the disaster.
In addition to the 1974 act, the Mines and Quarries (Tips) Act of 1969 and subsequent Mine and Quarries (Tips) Regulations of 1971 also brought standardization of mine building, construction, and management. According to the latter, any tipping activities required plans “showing all mine workings (whether abandoned or not), previous landslips, springs, artesian wells, watercourses and other natural and other topographical features which might affect the security of the intended tip or might be relevant for determining whether the land on which the tipping operations are to be carried out is satisfactory for the purpose.”
In 1999, additional quarry regulations were put into effect, tightening oversight of waste materials including, “but… not limited to, overburden dumps, backfill, spoil heaps, stock piles and lagoons.”
Families Impacted By The Disaster Were Paid £500 By The National Coal Board
A fund to support Aberfan and its community was established almost immediately after the disaster. A total of £1,750,000 – a sum worth more than £20 million today – was raised to rebuild the village and pay for medical care. Because the National Coal Board (NCB) refused to pay for the removal of the tips that still sat high above Aberfan, the money was used to bring those down, as well. In 1997, the British government repaid Aberfan the £150,000 from the fund that went toward the tip removal.
The NCB offered each of the families impacted by the disaster £50 as an opening payment, a sum that later rose to £500. The Charity Commission of the NCB once considered asking parents, “Exactly how close were you to your child?” before paying out – presumably, parents who were not close to their children would not receive compensation – but decided against that option. The “generous offer” of £500 was paid to the families in 1970.
Money would not cure the psychological scars in Aberfan, however. Survivor Jeff Edwards continues to struggle with survivor’s guilt, while families in Aberfan experienced a “strange bitterness between [those] who lost children and those who hadn’t; people just could not help it.” Post-traumatic stress disorder plagues the entire community and, while psychiatrists were initially brought in, “They didn’t really know how to deal with it and it wasn’t much help. There were sessions and we were offered different drugs.”
Thirty-three years after the disaster, researcher Louise Morgan found that survivors “talked about the fear evoked at the sound of a lorry passing their house, or of an aircraft flying overhead. Intense memories are aroused by the slightest noise or smell. A number now have children the age they were. This seems to arouse new feelings.”
The Queen Made Repeated Visits To Aberfan In Support Of The Community
Queen Elizabeth II may have received criticism for delaying a trip to Aberfan in 1966, but she has made numerous trips to the Welsh town in support of its recovery. In 1973, she visited to attend the opening of a new community center and placed a wreath at a local memorial. While there, she called the community center “a symbol of the determination that out of the disaster should come a richer and fuller life.”
When she returned in 1997, she planted a tree in the Garden of Remembrance, again speaking to survivors and relatives of those who perished.
Another visit in 2012 saw the queen opening a new school, something that, according to Elaine Richards, was part of a promise Elizabeth had made decades earlier. Richards, who lost her daughter Sylvie in 1966, noted, “She kept her promise, she is a very gracious lady… Now we have children playing in the village again.”
There is some research suggesting a link between being closeted and being anti-gay. But while the notion feeds many jokes, it also obscures very real homophobia.
Photo Illustration by The Daily Beast
2017 has been a banner year for the armchair psychological theory that anti-gay public figures are secretly gay themselves.
Never mind the long-running jokes and memes about Mike Pence covering up some secret homosexual identity. There have been actual examples this year of outspoken anti-LGBT figures exhibiting behavior that seems to contradict their political ideology.
The same idea emerges every time: The hypothesis is that their bigotry doesn’t just make their sexual behavior hypocritical, it actually functions as a cover for it, consciously or otherwise.
Recently, there has been former Ohio state Rep. Wesley Goodman, who resigned late last week after it came out that he had had sex with a man in his office.
In March, former Oklahoma state Sen. Ralph Shortey resigned after being hit with child prostitution charges for allegedly soliciting sex from a 17-year-old boy. Shortey has reportedly decided this week to plead guilty to a child sex trafficking charge.
Both Goodman and Shortey are married men who were clear political opponents of the LGBT community while in office.
After Shortey was arrested, the Associated Press noted that he “routinely” voted for anti-LGBT bills, quoting the director of the LGBT advocacy organization Freedom Oklahoma who said, “He was never vitriolic about it, but he would make the bad votes.”
More strident was Goodman who, as the Columbus Dispatch reported, “consistently touted his faith and conservative values,” with a Twitter bio that read: “Christian. American. Conservative. Republican.”
As more information about their alleged misdeeds emerges—Goodman now stands accused of fondling an 18-year-old man at a conservative event, and of pursuing several young gay men—there is a certain grim catharsis in seeing such hypocrisy exposed.
The LGBT community will never tire of bringing up the long history of Republican gay sex scandals every time new—and increasingly unsurprising—allegations emerge, precisely because they seem to be so predictable in hindsight.
(As GQ sarcastically put it in response to the Goodman news: “Anti-Gay Ohio Republican Resigns After, Surprise, Having Sex with a Man in the State Capitol.”)
A 2012 study in the Journal of Personality and Social Psychology generated a fair number of headlines that year—including The New York Times’ “Homophobic? Maybe You’re Gay”—for suggesting that some self-avowed straight people who showed signs of same-sex desire were more likely to hold discriminatory attitudes.
Two authors on the study—psychologists Richard M. Ryan and William S. Ryan—wrote in their accompanying New York Times opinion piece that they had asked 784 college students to rate their sexual orientation on a 10-point scale and then told them to sort “images and words indicative of hetero- and homosexuality” into categories.
The “twist,” as they put it, were subliminal flashes of the words “me” or “other” before each image that can theoretically reveal subconscious bias based on how long it takes the subjects to sort images that don’t match their self-described sexual identity into the right category.
The result: The researchers isolated a “subgroup of participants”—more than “20 percent of self-described highly straight individuals”—who “indicated some level of same-sex attraction,” and who were “significantly more likely than other participants to favor anti-gay policies; to be willing to assign significantly harsher punishments to perpetrators of petty crimes if they were presumed to be homosexual; and to express greater implicit hostility toward gay subjects.”
“Thus our research suggests that some who oppose homosexuality do tacitly harbor same-sex attraction,” they concluded.
The psychological mechanism behind this subgroup’s anti-LGBT vitriol is, in theory, relatively simple: They are taking out their own issues with sexual identity on other people.
As Netta Weinstein, the study’s lead author, said in a press release, they “may be threatened by gays and lesbians because homosexuals remind them of similar tendencies within themselves.” So if you’re an American politician, there may be no more effective way to prove to yourself that you’re straight than to target LGBT people.
The 2012 study is certainly suggestive. It’s continually cited whenever it seems to apply to a homophobic figure, like after Pulse nightclub gunman Omar Mateen was rumored to have frequented the LGBT nightclub in the buildup to the shooting.
There are other studies that have come to similar conclusions. As Science magazine reported after Pulse, there is a “scattering of research” that suggests “some conflicted gay men might indeed be homophobic,” like a small 1996 study in the Journal of Abnormal Psychology that measured penile arousal and found a link between “homophobia” and “homosexual arousal.”
But the keyword in all of the above literature is “some.”
There is, at this point, enough research in this area to suggest that there may be something deeper to the armchair psychology. But the “secretly gay homophobe” theory is far from being a complete explanation of anti-LGBT prejudice in American politics.
Twenty percent of people who describe themselves as “highly straight” is still 10 percent fewer than the 32 percent of Americans who oppose same-sex marriage.
Just because that 20-percent subgroup is “significantly more likely” to tout an anti-LGBT ideology doesn’t mean we can assume someone like Mike Pence is likely to be covering up a secret past as a gay clubgoer just because of his anti-LGBT track record. So-called closet cases may be abundant, but there’s no way to prove that every Republican who tries to legalize anti-LGBT discrimination is hiding something.
In fact, overgeneralizing and joking as if that were the case may hurt LGBT people.
On Twitter, comedian Cameron Esposito, herself a lesbian, has criticized the homophobic undertones of the constant Mike Pence jokes—and has called out the media for being seemingly more interested in the salacious “homophobe caught having gay sex” story than in the mistreatment of LGBT people writ large.
Throughout history, tales of brave, courageous people being executed for their beliefs, usually religious ones, are well known but the men who became known as the Tolpuddle Martyrs were not persecuted for their religion.
Tolpuddle is a village near Dorchester in Dorset, where in the years 1833 and 1834 a great wave of trade union activity took place and a lodge of the Friendly Society of Agricultural Labourers was established. Entry into the union involved payment of a shilling (5p) and swearing before a picture of a skeleton never to tell anyone the union’s secrets.
Lord Melbourne was Prime Minister at this time and he was bitterly opposed to the Trade Union Movement, so when six English farm labourers were sentenced in March 1834 to 7 years transportation to a penal colony in Australia for trade union activities, Lord Melbourne did not dispute the sentence.
The labourers were arrested ostensibly for administrating unlawful oaths, but the real reason was because they were trying to protest at their already pitiful wages. The labourers at Tolpuddle lived in meagre poverty on just 7 shillings a week and wanted an increase to 10 shillings, but instead their wages were cut to 6 shillings a week.
The Whig government had become alarmed at the working class discontent in the country at this time. The government and the landowners, led by James Frampton, were determined to squash the union and to control increasing outbreaks of dissent.
Six of the Tolpuddle labourers were arrested: George and James Loveless, James Brine, James Hammett, Thomas Stansfield and his son John. It was George Loveless who had established the Friendly Society of Agricultural Workers in Tolpuddle.
At their trial, the judge and jury were hostile and the six were sentenced to 7 years transportation to Australia. After the trial many public protest meetings were held and there was uproar throughout the country at this sentence, so the prisoners were hastily transported to Australia without delay.
The people were incensed at this treatment and after 250,000 people signed a petition and a procession of 30,000 people marched down Whitehall in support of the labourers, the sentences were remitted. After some delay, the the six were given a free passage home from Australia.
When finally home and free, some of the ‘martyrs’ settled on farms in England and four emigrated to Canada.
The tree under which the ‘martyrs’ met is now very old and reduced to a stump, but it has become a place of pilgrimage in Tolpuddle, where it is known as the ‘Martyrs Tree’. A commemorative seat and shelter was erected in 1934 on the green by the wealthy London draper Sir Ernest Debenham.
The story of the Tolpuddle Martyrs is perhaps the best known case in the early history of the Trade Union Movement.
A lot of people are saying this year’s midterm election is the most crucial of our lifetime. It may well be, given the need to elect officials who will fight Donald Trump’s loathsome agenda. But another midterm election, 40 years ago, was one of the most crucial as well, at least in California.
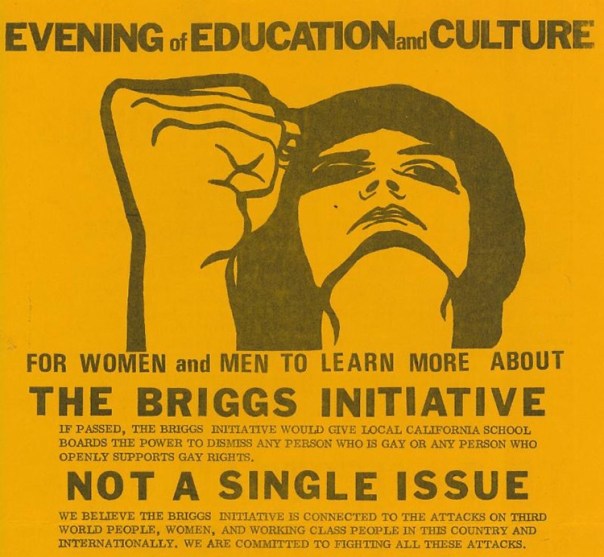
In 1978, State Sen. John Briggs put an initiative on the ballot that would have mandated the firing of any gay or lesbian teacher in California public schools, or any teacher who supported gay rights (the term LGBT wasn’t used back then). Thanks to a Herculean effort by California grassroots activists — Harvey Milk, Cleve Jones, Sally Miller Gearhart, hundreds of others — Briggs’s Proposition 6, popularly known as the Briggs Initiative, was resoundingly defeated, by more than a million votes. It was the first time voters had rejected an antigay measure.
To mark the 40th anniversary of this milestone, the GLBT Historical Society in San Francisco is mounting an exhibition called “The Briggs Initiative: A Scary Proposition,” recounting the story of the initiative and how it was turned back. It opens September 14.
“This exhibition will bring a scary time for LGBTQ people zinging back for those of us who were there, reminding us that we can fight the forces of anti-LGBTQ discrimination and win even against long odds,” said co-curator Sue Englander, a veteran of the anti-Briggs Initiative effort, in a press release. “And if you weren’t here 40 years ago, the story will sear itself into your consciousness. The differences between 1978 and today aren’t as big as they may look.”
Indeed, there are similarities between 1978 and today. The gay rights movement jump-started by the Stonewall riots and other events of the 1960s had made some gains in the 1970s. Gays and lesbians were getting elected to state- or city-level public office, or coming out and getting reelected — Elaine Noble in Massachusetts, Allan Spear in Minnesota, Harvey Milk in San Francisco. Many cities and counties, including San Francisco and Miami-Dade County, were adopting ordinances banning antigay discrimination. Major cities across the nation were holding Pride parades, usually around the anniversary of Stonewall in late June. The American Psychiatric Association announced it no longer considered homosexuality a mental illness.
This amount of progress pales in comparison with that of the 21st century, which brought nationwide marriage equality, many more antidiscrimination laws, and, for a time, a president who wholeheartedly supported LGBTQ equality. But just as the Trump administration and other anti-LGBTQ forces are trying to undo civil rights progress today, homophobes came out of the woodwork to try to strip away the advances of the 1970s. The Briggs Initiative was part of this backlash, as was Anita Bryant’s campaign to repeal the Miami-Dade County gay rights law. But where she succeeded, Briggs would fail.
Briggs was a far-right Republican from a district in Orange County, a conservative enclave between Los Angeles and San Diego. In a state that makes greater use of the citizen initiative process than almost any other that has it, he hoped Prop. 6 would boost his political career. Specifically, he aspired to become California’s governor.
But one of the forces who helped persuade voters to reject the initiative was a former governor — Ronald Reagan. When he became president a few years later, Reagan didn’t build a gay-friendly record — he courted the religious right and notoriously ignored the AIDS crisis. But in 1978, he announced his opposition to the Briggs Initiative in an informal letter and in responses to reporters’ questions, and on November 1, six days before the election, he published a commentary in the Los Angeles Herald-Examiner denouncing the measure.
“Whatever else it is, homosexuality is not a contagious disease like the measles,” he wrote. “Prevailing scientific opinion is that an individual’s sexuality is determined at a very early age and that a child’s teachers do not really influence this.” That language may sound pretty tepid now, but at the time it was a significant statement. Then-President Jimmy Carter and his predecessor, Gerald Ford, also opposed the initiative.
Opponents meet: John Briggs and Harvey Milk
But the credit for defeating the Briggs Initiative really should go not to high-profile politicians but to the many grassroots activists who worked against it. The opposition started with gay and lesbian advocates and the women’s movement, but they formed alliances with organized labor, progressive religious groups, and community organizations representing a variety of populations. Milk and Gearheart famously debated John Briggs, as chronicled in the documentary The Times of Harvey Milk and the narrative film Milk (although the latter left out Gearheart). They made mincemeat out of Briggs’s arguments, particularly about his initiative being a way to combat child molestation; Gearheart cited government data showing that this is overwhelmingly committed by straight men.
But most important, gay people came out. “We can defeat the Briggs Initiative if all the gay people come out to your family, your friends — if indeed they are your friends, your coworkers, your neighbors,” Milk said at the time. “You will hurt them if you come out, but think of how they will hurt you if they vote for Briggs. If they don’t come out, then it will be a very tight race.”
Indeed, gay people and their allies managed to flip the script on the initiative, as Ramy K. Khalil noted in his Western Washington University master’s thesis on the campaign. In August, just three months before the election, opinion polls showed support for the measure at 61 percent, opposition at 31 percent. By September, the polls showed a toss-up. And on November 7, voters delivered a resounding defeat, with the proposition losing by a margin of 58.4 percent to 41.6 percent, and not even carrying Briggs’s home county.
“One decisive factor was the mistake by Briggs himself of over-reaching — of promoting an initiative that was more extreme than the anti-gay ballot initiatives in other states,” Khalil wrote. “Proposition 6 required school districts to terminate employment of LGBT or straight people who expressed any sympathy toward homosexuality, on or off the job, whereas the ballot initiatives in other states merely repealed special protections against discrimination for gays or lesbians. Most importantly, though, Proposition 6 was defeated by LGBT people, labor unions, feminists, and other allies who organized a powerful grassroots movement involving highly visible protests and actions that successfully confronted the homophobic arguments behind Proposition 6.”
One of the posters to be featured in the exhibit“Never Again! Fight Back!” (San Francisco: Too Much Graphics, 1978); silk-screened poster sold as a fundraiser for the No on Six campaign, GLBT Historical Society.“No on 6” bumper sticker (San Francisco: Bay Area Committee Against the Briggs Initiative, 1978). Collection of the GLBT Historical Society.
The Briggs Initiative-A Scary Proposition GLBT Historical Society, September 2018 – January 2019, Curated by Sue Englander, Paula Lichtenberg, and Glenne McElhinney https://www.glbthistory.org/briggs
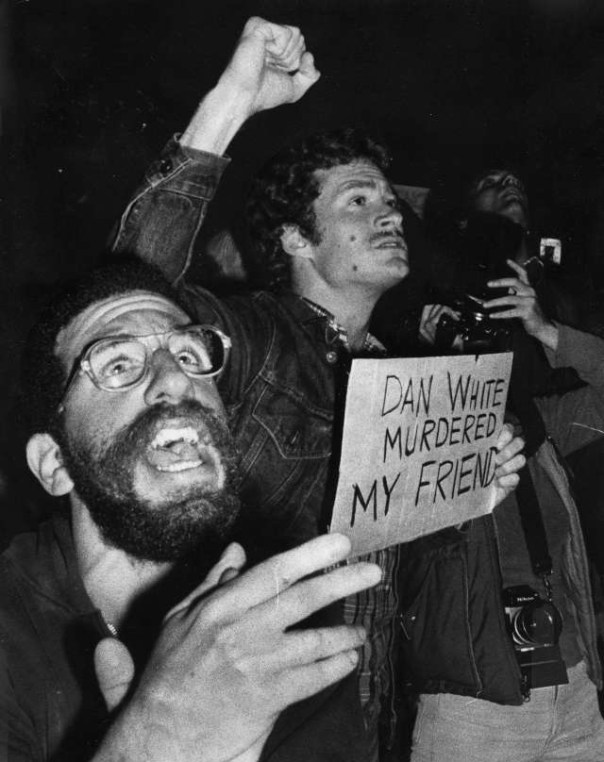
‘Dan White murdered my friend’: When anger boiled over into violence at City Hall and San Francisco police raided a Castro bar
On May 21, 1979, thousands of members of San Francisco’s predominantly gay Castro District community took to the streets to protest the lenient sentence received by Dan White for the murders of local politician and gay rights activist Harvey Milk and Mayor George Moscone. Their anger–combined with the actions of police who arrived to quell the scene–soon boiled over into rioting. The resulting violence affected San Francisco’s LGBT community for decades to come.
Harvey Milk rose to prominence as a gay rights activist and became the first openly gay person elected to a public office in the state of California when he was elected to the San Francisco Board of Supervisors in 1977. His murder, as well as that of Mayor Moscone, devastated not just the gay community, but the city as a whole.
Dan White was a former member of the Board of Supervisors who had clashed with Milk during their time serving the city together. In November of 1978, White resigned from his post, but changed his mind and asked to be reinstated. Mayor Moscone denied the request–with Milk lobbying against White’s reappointment. On November 27, White entered City Hall through a basement window and shot both men to death in their offices.
Six months later, White was convicted, not of first-degree murder, but voluntary manslaughter. White’s defense team had pointed to his diminished mental capacity and emotional state at the time of the murders, as indicated by the once-health conscious White consuming too much junk food– a ploy that became known as the “Twinkie Defense.” The jury-predominantly white, Roman Catholic and heterosexual—bought into it, recommending the lesser charge, which led to a sentence of just 7 years and 8 months.
When news of the verdict broke on the night of May 21, Cleve Jones–a close friend of Milk’s who would eventually go on to become one of the creators of the AIDS Quilt–spoke to a crowd of about 500 gatherers on Castro Street, and a peaceful march was quickly organized. By the time the crowd of protestors had made its second trip around the block, they were 1,500 strong. They then marched to City Hall, where their numbers expanded to an estimated 5,000.
As the crowd grew, so did the anger. Police soon arrived to try to control the situation, but that only served to enrage the crowd more. The police had raised over $100,000 for White’s defense–he was a former police officer–and many in the community believed the department had conspired to reduce White’s charges and sentencing. Although ordered to simply hold the crowd back, many officers began attacking the protestors with night sticks. Many had even taped over their badges, so as not to be identified.
Chaos erupted, as the crowd fought with police and destroyed a dozen police vehicles, as well as parts of City Hall itself. After three hours, officers moved in to quell the rioting for good, using tear gas in the process, and the crowd dispersed. In all, 59 officers and 124 protestors were injured, with about two dozen arrests made.
Hours later, several police officers gathered on their own to raid the Castro neighborhood, vandalizing a local bar and assaulting patrons. They shouted anti-gay slurs at the victims, and eventually turned their attention to attacking anyone that happened to be out on Castro Street.
After two hours, Police Chief Charles Gain was made aware of the rogue officers’ activities, and he made his way to the Castro to put a stop to it. No officers were reprimanded for the attacks, as officials were never able to determine who had ordered it, but the violence was finally over.
The next day, on what would have been Milk’s 49th birthday, 20,000 San Franciscans gathered to remember him. That October, more than 75,000 people marched for gay rights in Washington, D.C., and gay rights activists from around the country were inspired to continue their fight.
In San Francisco, the riots led to a wave of political changes, as more and more LGBT politicians were elected over the next decades. LGBT presence on the police forced also dramatically increased, and has continued to increase to this day.
There are still those out there who think AZT saved lives…it didn’t!I took it!I know!Will & Deni McIntyre—Getty Images
Today, if someone is diagnosed with HIV, he or she can choose among 41 drugs that can treat the disease. And there’s a good chance that with the right combination, given at the right time, the drugs can keep HIV levels so low that the person never gets sick.
That wasn’t always the case. It took seven years after HIV was first discovered before the first drug to fight it was approved by the U.S. Food and Drug Administration (FDA). In those first anxious years of the epidemic, millions were infected. Only a few thousand had died at that point, but public health officials were racing to keep that death rate from spiking — the inevitable result if people who tested positive weren’t treated with something.
As it turned out, their first weapon against HIV wasn’t a new compound scientists had to develop from scratch — it was one that was already on the shelf, albeit abandoned. AZT, or azidothymidine, was originally developed in the 1960s by a U.S. researcher as way to thwart cancer; the compound was supposed to insert itself into the DNA of a cancer cell and mess with its ability to replicate and produce more tumor cells. But it didn’t work when it was tested in mice and was put aside.
Two decades later, after AIDS emerged as new infectious disease, the pharmaceutical company Burroughs Wellcome, already known for its antiviral drugs, began a massive test of potential anti-HIV agents, hoping to find anything that might work against this new viral foe. Among the things tested was something called Compound S, a re-made version of the original AZT. When it was throw into a dish with animal cells infected with HIV, it seemed to block the virus’ activity.
The company sent samples to the FDA and the National Cancer Institute, where Dr. Samuel Broder, who headed the agency, realized the significance of the discovery. But simply having a compound that could work against HIV wasn’t enough. In order to make it available to the estimated millions who were infected, researchers had to be sure that it was safe and that it would indeed stop HIV in some way, even if it didn’t cure people of their infection. At the time, such tests, overseen by the FDA, took eight to 10 years.
Patients couldn’t wait that long. Under enormous public pressure, the FDA’s review of AZT was fast tracked — some say at the expense of patients.
Scientists quickly injected AZT into patients. The first goal was to see whether it was safe — and, though it did cause side effects (including severe intestinal problems, damage to the immune system, nausea, vomiting and headaches) it was deemed relatively safe. But they also had to test the compound’s effectiveness. In order to do so, a controversial trial was launched with nearly 300 people who had been diagnosed with AIDS. The plan was to randomly assign the participants to take capsules of the agent or a sugar pill for six months. Neither the doctor nor the patient would know whether they were on the drug or not.
After 16 weeks, Burroughs Wellcome announced that they were stopping the trial because there was strong evidence that the compound appeared to be working. One group had only one death. Even in that short period, the other group had 19. The company reasoned that it wouldn’t be ethical to continue the trial and deprive one group of a potentially life-saving treatment.
Those results — and AZT — were heralded as a “breakthrough” and “the light at the end of the tunnel” by the company, and pushed the FDA approve the first AIDS medication on March 19, 1987, in a record 20 months.
But the study remains controversial. Reports surfaced soon after that the results may have been skewed since doctors weren’t provided with a standard way of treating the other problems associated with AIDS — pneumonia, diarrhea and other symptoms — which makes determining whether the AZT alone was responsible for the dramatic results nearly impossible. For example, some patients received blood transfusions to help their immune systems; introducing new, healthy blood and immune cells could have helped these patients battle the virus better. There were also stories of patients from the 12 centers where the study was conducted pooling their pills, to better the chances that they would get at least some of the drug rather than just placebos.
And there were still plenty of questions left unanswered about the drug when it was approved. How long did the apparent benefits last? Could people who weren’t sick yet still benefit? Did they benefit more than those further along in their disease?
Such uncertainty would not be acceptable with a traditional approval, but the urgent need to have something in hand to fight the growing epidemic forced FDA’s hand. The people in the trial were already pressuring the company and the FDA to simply release the drug — if there were something that worked against HIV, they said, then it was not ethical to withhold it.
The drug’s approval remains controversial to this day, but in a world where treatment options are so far advanced it can be hard to imagine the sense of urgency and the social pressure permeating the medical community at the time. AIDS was an impending wave that was about to crash on the shores of an unsuspecting — and woefully unprepared — populace. Having at least one drug that worked, in however limited a way, was seen as progress.
But even after AZT’s approval, activists and public health officials raised concerns about the price of the drug. At about $8,000 a year (more than $17,000 in today’s dollars) — it was prohibitive to many uninsured patients and AIDS advocates accused Burroughs Wellcome of exploiting an already vulnerable patient population.
In the years since, it’s become clear that no single drug is the answer to fighting HIV. People taking AZT soon began showing rising virus levels — but the virus was no longer the same, having mutated to resist the drug. More drugs were needed, and AIDS advocates criticized the FDA for not moving quickly enough to approve additional medications. And side effects including heart problems, weight issues and more reminded people that anything designed to battle a virus like HIV was toxic.
Today, there are several classes of HIV drugs, each designed to block the virus at specific points in its life cycle. Used in combination, they have the best chance of keeping HIV at bay, lowering the virus’s ability to reproduce and infect, and ultimately, to cause death. These so-called antiretroviral drugs have made it possible for people diagnosed with HIV to live long and relatively healthy lives, as long they continue to take the medications.
And for most of these people, their therapy often still includes AZT.
AIDS HOPES DASHED BY TERRIBLE TRUTH ON AZT
It was the drug that held out hope to people carrying the world’s most feared virus. It had the power to move share prices by millions. What it could not do was help people facing AIDS.
This weekend the truth about AZT is in the open: a comprehensive trial, so big it equals all the other research put together, shows that the drug which dominates AIDS treatment has no effect in delaying the onset of the disease. After all the promise and the profits, AZT has nothing to offer people with HIV.
The findings came in the final report on the Anglo-French Concorde trial, published yesterday in The Lancet. Some 1,749 patients with HIV, but who showed no symptoms, were given either the drug or a placebo. There was no statistical difference in the progress of the two groups: after three years 18% had AIDS or were dead.
The results leave a terrible void for the 12m people worldwide said to be infected with the virus, and crush any remaining hopes that AZT might delay the onset of symptoms. They also raise questions as to how those hopes were fuelled in the first place.
Doubts about AZT were first revealed by The Sunday Times five years ago. A painstaking investigation showed that AZT had been rushed to market on the back of a flawed study that was supposed to demonstrate its effectiveness.
The American Food and Drug Administration (FDA), responsible for protecting the public from risk, had been aware of flaws in the trial, but gave AZT approval. Documents obtained under the American Freedom of Information Act showed that records compiled during the trial had been altered, giving the drug a more favourable record; “multiple deviations” from the terms of the study had occurred; and FDA investigators had argued for data from one centre to be dropped entirely from the results. A senior FDA official believed AZT should not be granted a licence, but was overruled.
The doubts did nothing to inhibit Wellcome, AZT’s maker, from promoting its drug. Patients with HIV, but without AIDS symptoms, were the new target. They are worth more money because there are more of them and because they have longer to live.
To show the drug’s usefulness to this lucrative group, Wellcome trumpeted a big American trial called Protocol 019. The trial was halted in August 1989, after less than two years, on the grounds that it had already shown such benefit to HIV-positive people it would be unethical not to give the drug to all who wanted it.
Such “benefit” was judged only by time free from disease. A new analysis of the trial data, however, reaches a similar conclusion to Concorde: that AZT is essentially useless.
The original results were announced with a fanfare by the National Institute of Allergy and Infectious Diseases, which sponsored it with Wellcome’s support. In London, The Independent newspaper gave its front page to the findings, under the headline “AIDS drug offers lease of life”.
The very different picture painted by last month’s analysis, in the New England Journal of Medicine, comes after investigators paid more attention to the drug’s side-effects. These can include anaemia, liver damage, fatigue, nausea, headaches and sometimes a collapse in white blood cells, making patients more prone to disease.
The researchers looked at the average time patients experienced neither a progression of disease nor an adverse effect. Those treated with low doses of AZT were found to suffer a reduction in quality of life “due to severe side-effects of therapy” that approximately equalled any benefit from slowing down the disease; people on higher doses suffered even greater side-effects, outweighing the supposed benefit.
Dr Peter Duesberg, the American virus expert who has claimed for years that AZT is not a rational therapy, says it is clear that the original claims were completely ill-founded. “The opposite interpretations of the same data lead me to conclude that those responsible are not acting as scientists; they are acting as politicians.
“When the time is ripe to say that AZT is detrimental, that it actually hurts, the interpretation will change again.”
For patients with AIDS-related symptoms, AZT will continue to be prescribed: the consensus remains that it gives a temporary benefit.
For those without symptoms, hope centres on combinations of drugs, or on other approaches such as gene therapy. However, Professor Ian Weller, of the Middlesex hospital in London, who was the principal British investigator in the Concorde trial, is alarmed by the drive to give AIDS patients an AZT drug cocktail as if it were already an established therapy.
“There’s a suspicion of more toxicity if you combine it with other treatment, and we are a long way from showing an important clinical benefit, or that it is safer than AZT on its own,” he said. “There are physicians who are jumping the gun.”
As late as Thursday, Wellcome was insisting that AZT “remains the best weapon we have to slow the progress of the disease”. Dr Trevor Jones, its research director, said: “The question is where in the course of the disease you begin.” *
AIDS and the AZT Scandal: SPIN’s 1989 Feature, ‘Sins of Omission’
The story of AZT, one of the most toxic, expensive, and controversial drugs in the history of medicine
At the end of 1989, two years after we had started the highly controversial AIDS column in SPIN, we published an article by Celia Farber called “Sins of Omission” about the truly bad and corrupt science surrounding promoting AZT as a treatment for the syndrome of diseases.
Celia was the editor and frequent writer of the column and unearthed hard evidence of the cold-bloodedness of the AIDS establishment pushing a drug that was worse than the disease, and killed faster than the natural progression of AIDS left untreated. AZT had been an abandoned cancer drug, discarded because of it’s fatal toxicity, resurrected in the cynical belief that AIDS patients were going to die anyway, so trying it out was sort of like playing with the house’s money. Because the drug didn’t require the usual massively expensive research and trial processes, having gone through that years earlier, it was insanely profitable for its maker, Burroughs Wellcome. It was a tragically perfect storm of windfall profits, something to pacify AIDS activists and the media, and a convenient boom to the patent holders for HIV testing.
Celia — who should get the Congressional Medal of Honor for her brave and relentless reporting, here and throughout the ten years we ran the column — exposed the worthlessness of the drug, the shady studies and deals to suppress the negative findings, and its awful and final consequences. This piece very literally changed the media’s view of AIDS and sharpened their discerning and skeptical eye. And soon after, AZT was once again shelved, hopefully this time forever.
Many times over the years since, people have come up to me and said that reading this article saved their lives, that they either stopped taking the drug and their health improved vastly, or they never took it because of what we reported. Nothing ever made me prouder.
— Bob Guccione Jr., founder of SPIN, October 3, 2015
[This story was originally published in the November 1989 issue of SPIN. In honor of SPIN’s 30th anniversary, we’ve republished this piece as part of our ongoing “30 Years, 30 Stories” series.]
On a cold January day in 1987, inside one of the brightly-lit meeting rooms of the monstrous FDA building, a panel of 11 top AIDS doctors pondered a very difficult decision. They had been asked by the FDA to consider giving lightning-quick approval to a highly toxic drug about which there was very little information. Clinically called Zidovudine, but nicknamed AZT after its components, the drug was said to have shown a dramatic effect on the survival of AIDS patients. The study that had brought the panel together had set the medical community abuzz. It was the first flicker of hope — people were dying much faster on the placebo than on the drug.
But there were tremendous concerns about the new drug. It had actually been developed a quarter of a century earlier as a cancer chemotherapy, but was shelved and forgotten because it was so toxic, very expensive to produce, and totally ineffective against cancer. Powerful, but unspecific, the drug was not selective in its cell destruction.
Drug companies around the world were sifting through hundreds of compounds in the race to find a cure, or at least a treatment, for AIDS. Burroughs Wellcome, a subsidiary of Wellcome, a British drug company, emerged as the winner. By chance, they sent the failed cancer drug, then known as Compound S, to the National Cancer Institute along with many others to see if it could slay the AIDS dragon, HIV. In the test tube at least, it did. At the meeting, there was a lot of uncertainty and discomfort with AZT. The doctors who had been consulted knew that the study was flawed and that the long-range effects were completely unknown. But the public was almost literally baying at the door. Understandably, there was immense pressure on the FDA to approve AZT, considering the climate of fear and anger all around.*
Everybody was worried about this one. To approve it, said Ellen Cooper, an FDA director, would represent a “significant and potentially dangerous departure from our normal toxicology requirements.” Just before approving the drug, one doctor on the panel, Calvin Kunin, summed up their dilemma. “On the one hand,” he said, “to deny a drug which decreases mortality in a population such as this would be inappropriate. On the other hand, to use this drug widely, for areas where efficacy has not been demonstrated, with a potentially toxic agent, might be disastrous.”
“We do not know what will happen a year from now,” said panel chairman Dr. Itzhak Brook. “The data is just too premature, and the statistics are not really well done. The drug could actually be detrimental.” A little later, he said he was also “struck by the fact that AZT does not stop deaths. Even those who were switched to AZT still kept dying.”
“I agree with you,” answered another panel member, “there are so many unknowns. Once a drug is approved, there is no telling how it could be abused. There’s no going back.” Burroughs Wellcome reassured the panel that they would provide detailed two-year follow-up data, and that they would not let the drug get out of its intended parameters: as a stopgap measure for very sick patients.
Dr. Brook was not won over by the promise. “If we approve it today, there will not be much data. There will be a promise of data,” he predicted, “but then the production of data will be hampered.” Brook’s vote was the only one cast against approval.
“There was not enough data, not enough follow-up,” Brook recalls. “Many of the questions we asked the company were answered by, ‘We have not analyzed the data yet,’ or, ‘We do not know.’ I felt that there was some promising data, but was very worried about the price being paid for it. The side effects were so very severe. It was chemotherapy. Patients were going to need blood transfusions, that’s very serious.”
“The committee was tending to agree with me,” says Brook, “that we should wait a little bit, be more cautious. But once the FDA realized we were intending to reject it, they applied political pressure. At about 4 p.m., the head of the FDA’s Center for Drugs and Biologics asked permission to speak, which is extremely unusual. Usually they leave us alone. But he said to us, ‘Look, if you approve the drug, we can assure you that we will work together with Burroughs Wellcome and make sure the drug is given to the right people.’ It was like saying ‘please do it.’”
Brad Stone, FDA press officer, was at that meeting. He says he doesn’t recall that particular speech, but that there is nothing “unusual” about FDA officials making such speeches at advisory meetings. “There was no political pressure,” he says. “The people in that meeting approved the drug because the data the company had produced proved it was prolonging life. Sure it was toxic, but they concluded that the benefits clearly outweighed the risks.” The meeting ended. AZT, which several members of the panel still felt uncomfortable with and feared could be a time bomb, was approved.
Flash forward: August 17, 1989. Newspapers across America banner-headlined that AZT had been “proven to be effective in HIV antibody-positive, asymptomatic, and early ARC patients,” even though one of the panel’s main concerns was that the drug should only be used in a last-case scenario for critically-ill AIDS patients, due to the drug’s extreme toxicity. Dr. Anthony Fauci, head of the National Institutes of Health (NIH), was now pushing to expand prescription.
The FDA’s traditional concern had been thrown to the wind. Already the drug had spread to 60 countries and an estimated 20,000 people. Not only had no new evidence allayed the initial concerns of the panel, but the follow-up data, as Dr. Brook predicted, had fallen by the wayside. The beneficial effects of the drug had proven to be temporary. The toxicity, however, stayed the same.
The majority of those in the AIDS-afflicted and medical communities held the drug up as the first breakthrough on AIDS. For better or worse, AZT had been approved faster than any drug in FDA history, and activists considered it a victory. The price paid for the victory, however, was that almost all government drug trials, from then on, focused on AZT — while over 100 other promising drugs were left uninvestigated.
Burroughs Wellcome stock went through the roof when the announcement was made. At a price of $8.000 per patient per year (not including blood-work and transfusions), AZT is the most expensive drug ever marketed. Burroughs Wellcome’s gross profits for next year are estimated at $230 million. Stock market analysts predict that Burroughs Wellcome may be selling as much as $2 billion worth of AZT, under the brand name Retrovir, each year by the mid-1990s — matching Burroughs Wellcome’s total sales for all its products last year.
“Does AZT do anything? Yes, it does. But the evidence that it does something against HIV is really not there.”
AZT is the only antiretroviral drug that has received FDA approval for treatment of AIDS since the epidemic began ten years ago, and the decision to approve it was based on a single study that has long been declared invalid. The study was intended to be a “double-blind placebo-controlled study,” the only kind of study that can effectively prove whether or not a drug works. In such a study, neither patient nor doctor is supposed to know if the patient is getting the drug or a placebo. In the case of AZT, the study became unblinded on all sides, after just a few weeks.
Both sides contributed to the unblinding. It became obvious to doctors who was getting what because AZT causes such severe side effects that AIDS per se does not. Furthermore, a routine blood count known as a CMV, which clearly shows who is on the drug and who is not, wasn’t whited out in the reports. Both of these facts were accepted and confirmed by both the FDA and Burroughs Wellcome, who conducted the study.
Many of the patients who were in the trial admitted that they had analyzed their capsules to find out whether they were getting the drug. If they weren’t, some bought the drug on the underground market. Also, the pills were supposed to be indistinguishable by taste, but they were not. Although this was corrected early on, the damage was already done. There were also reports that patients were pooling pills out of solidarity to each other. The study was so severely flawed that its conclusions must be considered, by the most basic scientific standards, unproven.
The most serious problem with the original study, however, is that it was never completed. Seventeen weeks into the study, when more patients had died in the placebo group, the study was stopped, five months prematurely, for “ethical” reasons: It was considered unethical to keep giving people a placebo when the drug might keep them alive longer. Because the study was stopped short, and all subjects were put on AZT, no scientific study can ever be conducted to prove unequivocally whether AZT does prolong life.
Dr. Brook, who voted against approval, warned at the time that AZT, being the only drug available for doctors to prescribe to AIDS patients, would probably have a runaway effect. Approving it prematurely, he said, would be like “letting the genie out of the bottle.”
Brook pointed out that since the drug is a form of chemotherapy, it should only be prescribed by doctors who have experience with chemotherapeutic drugs. Because of the most severe toxic effect of AZT — cell depletion of the bone marrow —patients would need frequent blood transfusions. As it happened, AZT was rampantly prescribed as soon as it was released, way beyond its purported parameters. The worst-case scenario had come true: Doctors interviewed by the New York Times later in 1987 revealed that they were already giving AZT to healthy people who had tested positive for antibodies to HIV.
The FDA’s function is to weigh a drug’s efficacy against its potential hazards. The equation is simple and obvious: A drug must unquestionably repair more than it damages, otherwise the drug itself may cause more harm than the disease it is supposed to fight. Exactly what many doctors and scientists fear is happening with AZT.
“I personally do not prescribe AZT. I have continued to experience that people live longer who are not on it.”
AZT was singled out among hundreds of compounds when Dr. Sam Broder, the head of the National Cancer Institute (NCI), found that it “inhibited HIV viral replication in vitro.” AIDS is considered a condition of immune suppression caused by the HIV virus replicating and eating its way into T-4 cells, which are essential to the immune system. HIV is a retrovirus which contains an enzyme called reverse transcriptase that converts viral RNA to DNA. AZT was thought to work by interrupting this DNA synthesis, thus stopping further replication of the virus.
While it was always known that the drug was exceedingly toxic, the first study concluded that “the risk/benefit ratio was in favor of the patient.”
In the study that won FDA approval for AZT, the one fact that swayed the panel of judges was that the AZT group outlived the placebo group by what appeared to be a landslide. The ace card of the study, the one that canceled out the issue of the drug’s enormous toxicity, was that 19 persons had died in the placebo group and only one in the AZT group. The AZT recipients were also showing a lower incidence of opportunistic infections.
While this data staggered the panel that approved the drug, other scientists insisted that it meant nothing — because it was so shabbily gathered, and because of the unblinding. Shortly after the study was stopped, the death rate accelerated in the AZT group. “There was no great difference after a while,” says Dr. Brook, “between the treated and the untreated group.”
“That study was so sloppily done that it really didn’t mean much,” says Dr. Joseph Sonnabend, a leading New York City AIDS doctor. Dr. Harvey Bialy, scientific editor of the journal Biotechnology, is stunned by the low quality of science surrounding AIDS research. When asked if he had seen any evidence of the claims made for AZT, that it “prolongs life” in AIDS patients, Bialy said, “No, I have not seen a published study that is rigorously done, analyzed, and objectively reported.”
Bialy, who is also a molecular biologist, is horrified by the widespread use of AZT, not just because it is toxic, but because, he insists, the claims its widespread use are based upon are false. “I can’t see how this drug could be doing anything other than making people very sick,” he says.
The scientific facts about AZT and AIDS are indeed astonishing. Most ironically, the drug has been found to accelerate the very process it was said to prevent: the loss of T-4 cells.
“Undeniably, AZT kills T-4 cells [white blood cells vital to the immune system],” says Bialy. “No one can argue with that. AZT is a chain-terminating nucleotide, which means that it stops DNA replication. It seeks out any cell that is engaged in DNA replication and kills it. The place where most of this replication is taking place is in the bone marrow. That’s why the most common and severe side effect of the drug is bone marrow toxicity. That is why they [patients] need blood transfusions.”
AZT has been aggressively and repeatedly marketed as a drug that prolongs survival in AIDS patients because it stops the HIV virus from replicating and spreading to healthy cells. But, says Bialy: “There is no good evidence that HIV actively replicates in a person with AIDS, and if there isn’t much HIV replication to stop, it’s mostly killing healthy cells.”
University of California at Berkeley scientist Dr. Peter Duesberg drew the same conclusion in a paper published in Proceedings, the journal of the National Academy of Sciences. Duesberg, whose paper addressed his contention that HIV is not a sufficient cause for AIDS, wrote: “Even if HIV were to cause AIDS, it would hardly be a legitimate target for AZT therapy, because in 70 to 100 percent of antibody-positive persons, proviral DNA is not detectable… and its biosynthesis has never been observed.”
As a chemotherapeutic drug, explained Duesberg, AZT “kills dividing blood cells and other cells,” and is thus “directly immunosuppressive.”
“The cell is almost a million-fold bigger target than the virus, so the cell will be much, much more sensitive,” says Duesberg. “Only very few cells, about one in 10,000, are actively making the virus containing DNA, so you must kill incredibly large numbers of cells to inhibit the virus. This kind of treatment could only theoretically help if you have a massive infection, which is not the case with AIDS. Meanwhile, they’re giving this drug that ends up killing millions of lymphocytes [white blood cells]. It’s beyond me how that could possibly be beneficial.”
“It doesn’t really kill them,” Burroughs Wellcome scientist Sandra Lehrman argues. “You don’t necessarily have to destroy the cell, you can just change the function of it. Furthermore, while the early data said that only very few cells were infected, new data says that there may be more cells infected. We have more sensitive detection techniques now.”
“Changes their function? From what — functioning to not functioning? Another example of mediocre science,” says Bialy. “The ‘sensitive detection technique’ to which Dr. Lehrman refers, PCR, is a notoriously unreliable one upon which to base quantitative conclusions.”
When specific questions about the alleged mechanisms of AZT are asked, the answers are long, contradictory, and riddled with unknowns. Every scientific point raised about the drug is eventually answered with the blanket response, “The drug is not perfect, but it’s all we have right now.” About the depletion of T-4 cells and other white cells, Lehrman says, “We don’t know why T-4 cells go up at first, and then go down. That is one of the drug mechanisms that we are trying to understand.”
When promoters of AZT are pressed on key scientific points, whether at the NIH, FDA, Burroughs Wellcome, or an AIDS organization, they often become angry. The idea that the drug is “doing something,” even though this is invariably followed with irritable admissions that there are “mechanisms about the drug and disease we don’t understand,” is desperately clung to. It is as if, in the eye of the AIDS storm, the official, government-agency sanctioned position is immunized against critique. Skepticism and challenge, so essential to scientific progress and so prevalent in every other area of scientific endeavor, is not welcome in the AZT debate, where it is arguably needed more than anywhere else.
The results, finally and ironically, are what damns AZT.
The toxic effects of AZT, particularly bone marrow suppression and anemia, are so severe that up to 50 percent of all AIDS and ARC patients cannot tolerate it and have to be taken off it. In the approval letter that Burroughs Wellcome sent to the FDA, all of 50 additional side effects of AZT, aside from the most common ones, were listed. These included: loss of mental acuity, muscle spasms, rectal bleeding, and tremors.
Anemia, one of AZT’s common side effects, is the depletion of red blood cells, and, according to Duesberg, “Red blood cells are the one thing you cannot do without. Without red cells, you cannot pick up ???gen.”
Fred, a person with AIDS, was put on AZT and suffered such severe anemia from the drug he had to be taken off it. In an interview in the AIDS handbook Surviving and Thriving With AIDS, he described what anemia feels like to editor Michael Callen: “I live in a studio and my bathroom is a mere five-step walk from my bed. I would just lie there for two hours; I couldn’t get up to take those five steps. When I was taken to the hospital, I had to have someone come over to dress me. It’s that kind of severe fatigue. The quality of my life was pitiful… I’ve never felt so bad… I stopped the AZT and the mental confusion, the headaches, the pains in the neck, the nausea, all disappeared within a 24-hour period.”
“I feel very good at this point,” Fred went on. “I feel like the quality of my life was a disaster two weeks ago. And it really was causing a great amount of fear in me, to the point where I was taking sleeping pills to calm down. I was so worried. I would totally lose track of what I was saying in the middle of a sentence. I would lose my directions on the street.”
“Many AIDS patients are anemic even before they receive the drug,” says Burroughs Wellcome’s Dr. Lehrman, “because HIV itself can infect the bone marrow and cause anemia.”
This argument betrays a bizarre reasoning. If AIDS patients are already burdened with problems such as immune suppression, bone marrow toxicity, and anemia, is compounding these problems an improvement?
“Yes, AZT is a form of chemotherapy,” says the man who invented the compound a quarter-century ago, Jerome Horwitz. “It is cytotoxic, and as such, it causes bone marrow toxicity and anemia. There are problems with the drug. It’s not perfect. But I don’t think anybody would agree that AZT is of no use. People can holler from now until doomsday that it is toxic, but you have to go with the results.”
The results, finally and ironically, are what damns AZT. Several studies on the clinical effects of AZT — including the one that Burroughs Wellcome’s approval was based on — have drawn the same conclusion: that AZT is effective for a few months, but that its effect drops off sharply after that. Even the original AZT study showed that T-4 cells went up for a while and then plummeted. HIV levels went down, and then came back up. This fact was well-known when the advisory panel voted for approval. As panel member Dr. Stanley Lemon said in the meeting, “I am left with the nagging thought that after seeing several of these slides, that after 16 to 24 weeks — 12 to 16 weeks, I guess — the effect seems to be declining.”
A follow-up meeting, two weeks after the original Burroughs Wellcome study, was scheduled to discuss the long-range effects of AZT and the survival statistics. As one doctor present at that meeting in May 1988 recalls, “They hadn’t followed up the study. Anything that looked beneficial was gone within half a year. All they had were some survival statistics averaging 44 weeks. The p24 didn’t pan out and there no persistent improvement in T-4 cells.”
HIV levels in the blood are measured by an antigen called p24. Burroughs Wellcome made the claim that AZT lowered this level, that is, lowered the amount of HIV in the blood. At the first FDA meeting, Burroughs-Welcome emphasized how the drug had “lowered” the p24 levels; at the follow-up meeting they didn’t even mention it.
As that meeting was winding down, Dr. Michael Lange, head of the AIDS program at St. Luke’s-Roosevelt Hospital in New York spoke up about this. “The claim of AZT is made on the fact that it is supposed to have an antiviral effect,” he said to Burroughs Wellcome, “and on this we have seen no data at all… Since there is a report in the Lancet [a leading British medical journal] that after 20 weeks or so, in many patients p24 came back, do you have any data on that?”
They didn’t.
“What counts is the bottom line,” one of the scientists representing Burroughs Wellcome summed up, “the survival, the neurologic function, the absence of progression and the quality of life, all of which are better. Whether you call it better because of some antiviral effect, or some other antibacterial effect, they are still better.”
Dr. Lange suggested that the drug may be effective in the same way a simple anti-inflammatory, such as aspirin, is effective. An inexpensive, nontoxic drug called Indomecithin, he pointed out, might serve the same function, without the devastating side effects.
One leading AIDS researcher, who was part of the FDA approval process, says today: “Does AZT do anything? Yes, it does. But the evidence that it does something against HIV is really not there.”
“There have always been drugs that we use without knowing exactly how they work,” says Nobel Prize winner Walter Gilbert. “The really important thing to look at is the clinical effect. Is the drug helping or isn’t it?”
A physician with extensive experience with AIDS patients who asked to remain anonymous told SPIN, point blank: “I personally do not prescribe AZT. I have continued to experience that people live longer who are not on it.”
“I’m living proof that AZT works,” says one person with ARC on AZT. “I’ve been on it for two years now, and I’m certainly healthier than I was two years ago. It’s not a cure-all, it’s not a perfect drug, but it’s effective. It’s slowing down the progression of the disease.”
“Sometimes I fee like I’m swallowing Drano,” says another. “I mean, sometimes I have problems swallowing. I just don’t like the idea of taking something that foreign to my body. But every six hours, I’ve got to swallow it. Until something better comes along, this is what is available to me.”
“I am absolutely convinced that people enjoy a better quality of life and survive longer who do not take AZT,” says Gene Fedorko, President of Health Education AIDS Liaison (HEAL). “I think it’s horrible the way people are bullied by their doctors to take this drug. We get people coming to us shaking and crying because their doctors said they’ll die if they don’t take AZT. That is an absolute lie.” Fedorko has drawn his conclusion from years of listening to the stories of people struggling to survive AIDS at HEAL’s weekly support group.
“I wouldn’t take AZT if you paid me,” says Michael Callen, cofounder of New York City’s PWA coalition, Community Research Initiative, and editor of several AIDS journals. Callen has survived AIDS for over seven years without the help of AZT. “I’ve gotten the s–t kicked out of me for saying this, but I think using AZT is like aiming a thermonuclear warhead at a mosquito. The overwhelming majority of long-term survivors I’ve known have chosen not to take AZT.”
“I’m convinced that if you gave AZT to a perfectly healthy athlete he would be dead in five years.”
The last surviving patient from the original AZT trial, according Burroughs Wellcome, died recently. When he died, he had been on AZT for three and one-half years. He was the longest surviving AZT recipient. The longest surviving AIDS patient overall, not on AZT, has lived for eight and one-half years.
An informal study of long-term survivors of AIDS followed 24 long-term survivors, all of whom had survived AIDS for more than six years. Only one of them had recently begun taking AZT.
In the early days, AZT was said to extend lives. In actual fact, there is simply no solid evidence that AZT prolongs life.
“I think AZT does prolong life in most people,” says Dr. Bruce Montgomery of the State University of New York at Stony Brook, who is completing a study on AZT. “There are not very many long-term survivors, and we really don’t know why they survive. It could be luck. But most people are not so lucky.”
“AZT does seem to help many patients,” says Dr. Bernard Bahari, a New York City AIDS physician and researcher, “but it’s very hard to determine whether it actually prolongs life.”
“Many of the patients I see choose not to take AZT,” says Dr. Don Abrams of San Francisco General Hospital. “I’ve been impressed that survival and lifespan are increasing for all people with AIDS. I think it has a lot to do with aerosolized Pentamadine [a drug that treats pneumocystis carinii pneumonia]. There’s also the so-called plague effect, the fact that people get stronger and stronger when a disease hits a population. The patients I see today are not as fragile as the early patients were.”
“Whether you live or die with AIDS is a function of how well your doctor treats you, not of AZT,” says Dr. Joseph Sonnabend, one of New York City’s first and most reputable AIDS doctors, whose patients include many long-term survivors, although he has never prescribed AZT. Sonnabend was one of the first to make the simple observation that AIDS patients should be treated for their diseases, not just for their HIV infection.
Several studies have concluded that AZT has no effect on the two most common opportunistic AIDS infections, Pneumocystic Carinii Pneumonia (PCP) and Kaposi’s Sarcoma (KS). The overwhelming majority of AIDS patients die of PCP, for which there has been an effective treatment for decades. This year, the FDA finally approved aerosolized Pentamadine for AIDS. A recent Memorial Sloan Kettering study concluded the following: By 15 months, 80 percent of people on AZT not receiving Pentamadine had a recurrent episode of pneumocystis. Only 5 percent of those people who did get Pentamadine had a recurring episode. “All those deaths in the AZT study were treatable,” Sonnabend says. “They weren’t deaths from AIDS, they were deaths from treatable conditions. They didn’t even do any autopsies for that study. What kind of faith can one have in these people?”
“If there’s one resistance to AZT in the general public at all, it’s within the gay community of New York,” says the doctor close to the FDA approval, who asked to remain anonymous. “The rest of this country has been brainwashed into thinking this drug really does that much. The data has all been manipulated by people who have a lot vested in AZT.”
“If AIDS were not the popular disease that it is — the money-making and career-making machine — these people could not get away with this kind of shoddy science,” says Bialy. “In all my years in science I have never seen anything this atrocious.” When asked if he thought it was at all possible that people have been killed as a result of AZT poisoning rather than AIDS he answered: “It’s more than possible.”
August 17, 1989: The government has announced that 1.4 million healthy, HIV antibody-positive Americans could “benefit” from taking AZT, even though they show no symptoms of disease. New studies have “proven” that AZT is effective in stopping the progression of AIDS in asymptomatic and early ARC cases. Dr. Fauci, the head of NIH, proudly announced that a trial has been going on for “two years” had “clearly shown” that early intervention will keep AIDS at bay. Anyone who has antibodies to HIV and less than 500 T-4 cells should start taking AZT at once, he said. That is approximately 650,000 people. 1.4 million Americans are assumed HIV antibody-positive, and eventually all of them may need to take AZT so they don’t get sick, Fauci contended.
The leading newspapers didn’t seem to think it unusual that there was no existing copy of the study, but rather a breezy two-page press release from the NIH. When SPIN called the NIH asking for a copy of the study, we were told that it was “still being written.”
We asked a few questions about the numbers. According to the press release, 3,200 early ARC and asymptomatic patients were divided into two groups, one AZT and one placebo, and followed for two years. The two groups were distinguished by T-4 cell counts; one group had less than 500, the other more than 500. These two were then divided into three groups each: high-dose AZT, low-dose AZT, and placebo. In the group with more than 500 T-4 cells, AZT had no effect. In the other group, it was concluded that low-dose AZT was the most effective, followed by high-dose. All in all, 36 out of 900 developed AIDS in the two AZT groups combined, and 38 out of 450 in the placebo group. “HIV-positive are twice as likely to get AIDS if they don’t take AZT,” the press declared.
However, the figures are vastly misleading. When we asked how many patients were actually enrolled for a full two years, the NIH said they did not know, but that the average time of participation was one year, not two.
“It’s terribly dishonest the way they portrayed those numbers,” says Dr. Sonnabend. “If there were 60 people in the trial those numbers would mean something, but if you calculate what the percentage is out of 3,200, the difference becomes minute between the two groups. It’s nothing. It’s hit or miss, and they make it look like it’s terribly significant.”
The study boasted that AZT is much more effective and less toxic at one-third the dosage than has been used for three years now. That’s the good news. The bad news is that thousands have already been walloped with 1,500 milligrams of AZT and possibly even died of toxic poisoning — and now we’re hearing that one third of the dose would have done?
With all that remains so uncertain about the effects of AZT, it seems criminal to advocate expanding its usage to healthy people, particularly since only a minuscule percentage of the HIV-infected population have actually developed ARC or AIDS.
Burroughs Wellcome has already launched testing of AZT in asymptomatic hospital workers, pregnant women, and in children, who are getting liquid AZT. The liquid is left over from an aborted trial, and given to the children because they can mix it with water — children don’t like to swallow pills. It has also been proposed that AZT be given to people who do not yet even test positive for HIV antibodies, but are “at risk.”
“I’m convinced that if you gave AZT to a perfectly healthy athlete,” says Fedorko, “he would be dead in five years.”
“This is such shoddy science it’s hard to believe nobody is protesting.”
In December 1988, the Lancet published a study that Burroughs Wellcome and the NIH do not include in their press kits. It was more expansive than the original AZT study and followed patients longer. It was not conducted in the United States, but in France, at the Claude Bernard Hospital in Paris, and concluded the same things about AZT that Burroughs Wellcome’s study did, except Burroughs Wellcome called their results “overwhelmingly positive,” and the French doctors called theirs “disappointing.” The French study found, once again, that AZT was too toxic for most to tolerate, had no lasting effect on HIV blood levels, and left the patients with fewer T-4 cells than they started with. Although they noticed a clinical improvement at first, they concluded that “by six months, these values had returned to their pretreatment levels, and several opportunistic infections, malignancies, and deaths occurred.”
“Thus the benefits of AZT are limited to a few months for ARC and AIDS patients,” the French team concluded. After a few months, the study found, AZT was completely ineffective.
The news that AZT will soon be prescribed to asymptomatic people has left many leading AIDS doctors dumbfounded and furious. Every doctor and scientist I asked felt that it was highly unprofessional and reckless to announce a study with no data to look at, making recommendations with such drastic public health implications. “This simply does not happen,” says Bialy. “The government is reporting scientific facts before they’ve been reviewed? It’s unheard of.”
“It’s beyond belief,” says Dr. Sonnabend in a voice tinged with desperation. “I don’t know what to do. I have to go in and face an office full of people asking for AZT. I’m terrified. I don’t know what to do as a responsible physician. The first study was ridiculous. Margaret Fischl, who has done both of these studies, obviously doesn’t know the first thing about clinical trials. I don’t trust her. Or the others. They’re simply not good enough. We’re being held hostage by second-rate scientists. We let them get away with the first disaster; now they’re doing it again.”
“It’s a momentous decision to say to people, ‘If you’re HIV-positive and your T-4 cells are below 500, start taking AZT,’” says the AIDS doctor who wished to remain anonymous. “I know dozens of people that I’ve seen personally every few months for several years now who have been in that state for more than five years, and have not progressed to any disease.”
“I’m ashamed of my colleagues,” Sonnabend laments. “I’m embarrassed. This is such shoddy science it’s hard to believe nobody is protesting. Damned cowards. The name of the game is to protect your grant, don’t open your mouth. It’s all about money… it’s grounds for just following the party line and not being critical, when there are obviously financial and political forces driving this.”
When Duesberg heard the latest announcement, he was partially stunned over the reaction of Gay Men’s Health Crisis President Richard Dunne, who said that GMHC now urged “everybody to get tested,” and of course those who test positive to go on to AZT. “These people are running into the gas chambers,” says Duesberg. “Himmler would have been so happy if only the Jews were this cooperative.”
* = This sentence was changed to correct an error in the original version of this article, which wrongly stated that the FDA had approved Thalidomide.
The rise and fall of AZT: It was the drug that had to work. It brought hope to people with HIV and Aids, and millions for the company that developed it. It had to work. There was nothing else. But for many who used AZT – it didn’t
RUMOURS about the drug had been circulating since early 1985 when word came from America that a company in Carolina had found a compound that was effective against HIV – at least in a Petri dish. Two years later, by the time AZT had been licensed for use, demand for it had grown to gigantic proportions.
By then, Aids patients had grown so desperate that they would sample any of the bootlegged underground therapies, some of which were probably life-threatening. With the arrival of AZT, doctors who had been powerless for so long against a syndrome about which they knew so little, at last had something they could give their patients that had passed stringent official tests.
In March 1987, when AZT was available on prescription for the first time, almost everyone with Aids wanted to take it, as did many who had tested positive for HIV. One of these was Michael Cottrell, a gay Englishman. He had tested positive for HIV in 1985 at the age of 22. He took AZT for several months in the late Eighties and suffered severe side-effects from the drug: chronic headaches and nausea, debilitating muscle fatigue. Cottrell felt much worse on AZT than he did off it. But he persevered because it seemed AZT was the only anti-Aids drug there was.
So Cottrell took it early in his infection: after all, if AZT was judged to be effective in treating Aids, then perhaps, it was thought, it would also benefit those who took it before they became ill. AZT spelt hope: psychologically it served to dispel despair. It was never claimed to be a cure, but it did claim to keep you alive longer, and in that extra time it bought, who knew what would happen? Maybe a cure would be found. Maybe a vaccine. Maybe other drugs would be developed to fight the disease, too.
Cottrell still has boxes of AZT capsules at home. He gave up on it after several months, because he couldn’t stand how ill he was feeling on the drug; he felt as though his immune system was being damaged rather than strengthened; he believed he had never encountered a drug as toxic as AZT.
Cottrell knew the drug didn’t work for him, but he believed he might have been one of the unlucky ones, like people who react badly to penicillin. Then a month ago he woke up to the news that the drug didn’t work on HIV at all, and that all his suffering had been avoidable.
Concorde, an Anglo-French programme, was the biggest clinical trial of AZT ever conducted: 1,749 patients over three years. It did not examine how effective AZT was in treating people who were seriously ill with Aids but, just as important, it looked at how effective the drug was in treating the millions of people with HIV, before they became unwell and showed Aids symptoms. Preliminary results of the trial were published in a letter in the Lancet, and made headlines worldwide. The results suggested that early intervention with AZT – for people who were HIV but had not yet developed any symptoms of Aids – was a waste of time. The study, organised by the British Medical Research Council and the equivalent body in France, reported that it made no difference to either mortality rates or disease progression if one took AZT before the onset of Aids.
In a ‘blind’ test, AZT was given to 877 people and 872 were given a placebo. As soon as a patient developed any Aids symptoms, he or she (15 per cent were women) would be offered ‘open-label’ AZT. The mortality rates appeared to be shocking: over the three years of the trial, there were 79 Aids-related deaths in the AZT group, but only 67 in the placebo group. The researchers explained that among so many patients this figure was not statistically significant, but if you were HIV-positive and read of this in the newspapers, you were bound to question all the great claims that had been made for AZT. More people got Aids and died on Concorde than on any previous trial.
There were other causes for concern. Those on AZT developed more side-effects than those on the placebo. The results of the tests also cast doubt on one of the fundamental ways we measure a person’s immunity to disease. Those given AZT early increased their ‘CD4’ or ‘T4’ cell count; these are the cells attacked by HIV, and their numbers drop as the disease spreads. But the fact that, even with this higher count, patients did not live longer or develop the disease more slowly, struck at one of the basic tenets of Aids research.
Cottrell told the news to his 28-year-old partner Karl Burge, who had been diagnosed as HIV-positive four years ago, and they decided to take action. But what could they do? They had already joined protests against Wellcome plc, the British company that made AZT and had reaped millions in sales and share profits. Wellcome executives had listened to their complaints, and had admitted to certain levels of toxicity in AZT, but claimed that their product still had great beneficial effects. They were not readily going to halt production of the drug that last year made them pounds 213m, their second biggest earner.
So Cottrell and his friends selected a new target, the Terrence Higgins Trust. This was a strange choice: the trust, Britain’s most prominent Aids charity over the past 10 years, is staffed by dedicated professionals and volunteers providing a large range of support and information about all aspects of Aids and HIV; it developed the caring ‘buddy’ system; it produced information for schools; it sat on many Aids research panels and often met government departments.
So what had it done wrong? It had taken money from Wellcome plc and included positive information about AZT in its many leaflets and documents. Cottrell and his friends felt they were being betrayed by the very organisation that they had believed existed to act in their best interests; they felt that what was once an invaluable institution was acting as a mouthpiece for a multinational pharmaceuticals company.
Last week, Cottrell and Burge were still pitched outside the Terrence Higgins Trust office in central London, four weeks after their protest began. On Wednesday they were arrested and charged with a public order offence after a member of the trust called the police. The protest is growing by the week. They have been joined by John Stevens, diagnosed HIV- positive more than eight years ago, and who also had bad experiences with AZT, and Pierre Hardy, diagnosed HIV-positive four years ago when he was 27 and had felt devastated by its effects. Many other protesters carry placards, collect signatures, hand out leaflets. You will not find a more potent symbol of the complex story of AZT, a story of how the struggle to find a ‘magic bullet’ to help millions of people has degenerated into a saga of distrust, confusion, and anger. It is a story of health and illness, but it is also a story of scientific ambition, secrecy and political pressure, and of the amounts of money that can be generated when a lethal virus turns into a worldwide epidemic.
IN 1964, Jerome Horwitz was working in his laboratory at the Michigan Cancer Foundation when he had what he hoped was a brilliant idea. At 45, Dr Horwitz was the foundation’s director of chemistry, and although not in the scientific premier league, was a respected local researcher with his own lab and assistants. He had spent much of the previous decade doing what many of the world’s leading scientists had done – working on a cure, or at the very least an effective treatment, for cancer.
He developed a theoretical solution: what was needed was a chemical that would insert a ‘phoney’ compound into the DNA ‘building block’ of a cell to prevent its replication. After years of research, Dr Horwitz came up with
azidothymidine (AZT).
He tried his new compound on leukaemic mice, but it had no effect. Horwitz didn’t know why, but AZT didn’t work.
Horwitz never became famous. Recently he said AZT ‘was a terrible disappointment . . . we dumped it on the junkpile. I didn’t keep the notebooks.’ The compound remained ‘on the shelf’, occasionally tried by other researchers but always found to be useless. There was no reason to patent it. But 20 years later, Burroughs Wellcome brought it back to life.
THE WELLCOME group was founded in London by two Americans in 1880. Its first significant achievement was the creation of the tablet – previously most medication had been administered in powder form. In the 1930s the group was split into two distinct parts: the Wellcome Trust, a large charity which devoted its income to scientific research and the maintenance of an institute and library concerned with the history of medicine; and the Wellcome Foundation Ltd, a profit-making pharmaceuticals company that was called Burroughs Wellcome in the United States. In the course of its research, Wellcome employees have won five Nobel prizes.
By 1980, Wellcome had specialised in the treatment of viruses for more than 15 years, and its anti-viral drugs accounted for the bulk of its income. In that year, David Barry, a leading researcher at Burroughs Wellcome in the US, noticed that demand for its drug Septra – a drug that Wellcome had helped to develop a few years earlier to combat a rare form of pneumonia – was suddenly on the increase. Previously this pneumonia, known as PCP, was prevalent only in children with leukaemia, but now many doctors were requesting it for adult males. Most of these men were gay, and living in New York and San Francisco.
Two years later, another new Wellcome drug, Zovirax, was in great demand among the same group of people. Zovirax was an anti- herpes treatment. Dr Barry was very disturbed by the sudden demand for these two drugs.
Aids (Acquired Immune Deficiency Syndrome) was first classified as a new disease in 1981, but it was not until 1984 that the cause was identified as HIV (Human Immunodeficiency Virus). This cause has since been challenged by several prominent molecular biologists, but it remains the cornerstone of Aids research. And if any company was ideally equipped to conduct research into combating a new virus, it was Wellcome.
It was only natural for Barry to devote much of the company’s research resources to fight HIV. No one knew how widespread the virus or Aids was or would become. In 1984, only about 3,000 people had been diagnosed with Aids, but some early forecasts were terrifying: millions of people might already be infected, and hundreds of thousands could die within the next few years. Any scientist could see that Aids was potentially a career-making race to the Nobel prize. Millions might be made from a successful treatment.
After a few years of government inactivity – shameful years in which this new disease was virtually ignored – political ambition added to the desire to find a treatment. Health departments noticed that it wasn’t just homosexuals who were being struck down, but also hundreds of haemophiliacs and drug users. A certain amount of official panic took hold: by the time Rock Hudson died in the summer of 1985, it was clear that anyone – even film stars – could be in the frontline.
According to Wellcome’s own three-page account, research into HIV began in June 1984. During mass testing of scores of anti-viral
compounds, a substance known at first only as Compound S was found to inhibit viruses in animal cells. Compound S was AZT, a resyn- thesised version of what Horwitz had made 20 years before (Wellcome credits Horwitz in its account, but spells his name wrong).
In November 1984, according to the Wellcome account, the company sent samples of AZT to Duke University in North Carolina, the Food and Drug Administration (FDA) and the National Cancer Institute for independent testing, and within a few weeks the results confirmed what Wellcome already believed: that the stuff worked against HIV in test-tubes under laboratory conditions. Wellcome had already progressed further than Horwitz, but the real test – its effect on humans – was fraught with danger.
But first there is another account of the development of AZT to consider. A US government official named Sam Broder believes he has far more claim to being ‘Mr AZT’ than anyone at Burroughs Wellcome. Broder, the director of the National Cancer Institute, claims that Burroughs Wellcome showed little interest in developing an anti-Aids drug.
Broder went on a tour of pharmaceuticals companies towards the end of 1984, imploring them to send any possible anti-viral compounds to his lab for testing in safe conditions. ‘I went to one prestigious company, hat in hand,’ he told the business writer Bruce Nussbaum, whose book, Good Intentions, traces a history of the search for anti-Aids drugs. ‘I got about one minute and thirty seconds of a high-ranking officer’s time. It was very disappointing for me. It was emblematic of the issue. There was no real interest in it.’
Broder then went to Burroughs Wellcome. He says: ‘They made it clear that on the basis of 3,000 patients, there was no way they could practically get involved.’ Broder says he then became abrasive. ‘As I left, I said, ‘You know, we’re going to have more than 3,000 cases. It is going to be commercially viable for you . . .’ ‘
Whoever pushed who, the drug came through. When Broder found that the AZT sent to him by Burroughs Wellcome in November 1984 worked against the virus, he assured the company that every effort would be made to get this great new drug to dying patients as soon as possible. The FDA’s stringent testing requirements mean that most new drugs take between eight and 10 years to pass from development to the marketplace. AZT was pushed through in just 20 months.
This could have been the early history of almost any drug; the difference is, during what would normally have been an eight-year test period, for six of those years the drug was already on the market. At a time of desperation, this drug looked like the one that would restore hope. The National Cancer Institute had previously tried one other therapy, Suramin, which proved to be toxic in early tests, but AZT appeared to be far less poisonous. And so it was put on the ‘fast track’: the testing of some other drugs for less life-threatening illnesses was put aside; AZT was given top priority, an all-or-bust thing. But could any drug live up to the boundless hopes pinned on AZT?
THIS IS how AZT is supposed to work against HIV. HIV enters body cells, usually T4 white blood cells that play a crucial role in the orchestration of the body’s immune system. HIV is one of a group of viruses known as retro- viruses, which means that, unlike most living things that store their genetic information as DNA, HIV stores it as RNA. Before HIV can replicate, it must convert its RNA code to DNA by use of a special enzyme. It is during this conversion process that AZT works. When AZT enters the body, it is transformed into a molecule that closely resembles one of the building blocks of DNA. During the process of HIV conversion, this molecule is incorporated mistakenly into the DNA. The addition of this ‘phoney’ molecule makes the addition of further building blocks impossible and halts replication of the virus. It’s a form of chemotherapy. It worked fine under a microscope.
The first human tests were in two phases. The first examined whether AZT could be tolerated in the body at all, and whether it entered the brain, crossing the ‘blood-brain barrier’; to know this was important, because a common Aids symptom is dementia. The first Aids patient was injected with AZT in July 1985. This test concluded that the blood-brain barrier was crossed, and that although there were levels of toxicity detected, these were deemed to be safe.
The second phase of the tests, the final hurdle to the granting of a licence for mass production, was a shambles. It was set up six months later to establish whether AZT would combat Aids. This test, overseen by the Food and Drug Administration, involved 282 patients, all of them already ill with Aids or Arc (Aids-related complex). It was to be a placebo test, conducted over 24 months. It was to be a ‘double-blind’ study in which neither patient nor doctor knew whether the capsules being taken were AZT or starch. (But before the tests could begin, Wellcome had to produce large quantities of AZT, and found it couldn’t do it. It had run out of one crucial ingredient: herring sperm. Finally, Wellcome bought it in bulk from another company.)
At a press conference after the tests in September 1986, Wellcome reported that they had been a considerable success, such a success that the 24-week trial had been halted after 16 weeks for ‘ethical’ reasons. Mortality rates for people taking AZT were staggeringly lower than those taking the placebo; there had been 19 deaths in the placebo group of 137 people, but only one in the AZT group of 145. Those on AZT also had a decreased number of opportunistic infections and showed improvement in weight gain and T4 cell counts. Wellcome agreed in response to pressure from some sectors of the gay community that if AZT was effective, then dying people should be taken off the placebo at once.
No one claimed it was a cure, but there was huge relief that a breakthrough had been made. There had been much embarrassment when it became known that Rock Hudson had attended the Pasteur Institute in France for treatment; now at last America was showing those foreigners a thing or two. Robert Windom, assistant health secretary, said that ‘treatment with AZT prolongs survival of persons with Aids’. The results were ‘exciting’.
It was not suitable for everyone, but it was the best thing yet. In fact, it was the only thing. Last year, interviewed in the Wellcome in- house magazine, David Barry said that ‘the staff at Wellcome can tell our children, grandchildren and great-grandchildren that we were there, that we made a difference’. When it was shown that AZT worked, ‘we . . . first had a frenzied, cheerful celebration, and then a very quiet one. The longer we considered the global implications, the greater the accomplishment we realised Wellcome had made in the control of the HIV epidemic.’
But a few months after AZT was made available, John Lauritsen, a journalist working on the gay newspaper New York Native, obtained test documents through the Freedom of Information Act that suggested that many rules had been broken in the trials. The trial had been ‘unblinded’ within weeks: some patients claimed they could tell what they were taking by taste; others were so keen to have AZT that they pooled their treatment with other patients to increase their chances of receiving the drug. The documents showed that almost half the AZT patients had received numerous blood transfusions in the course of the trial, because of damage to their bone marrow and immune systems; and that a few had to be taken off AZT altogether.
What happened after the trial ended suggested something more alarming about AZT. After 16 weeks, one AZT patient was dead, compared to 19 placebo patients; a week later two more patients on AZT had died, compared to four more on the placebo. The ratio had switched from 19:1 to 23:3, which suggested AZT might only be effective for a limited time.
If the trial had continued, the ratio might have narrowed even more. The tests would probably still have shown that AZT has some benefits for very ill patients, but with hindsight it is alarming that a new drug was allowed to be
released with so much left to prove. People at Wellcome now put it down to the mood and the severe pressure of the times. Dr Trevor Jones, Director of Research at Wellcome, who has been involved in their development of AZT from the beginning, acknowledged that the trials were subject to extraordinary pressures. ‘Much of these accusations (about the breakdown of trial protocol) took place, not at that stage, but later on, when the drug was showing benefit in a less sick population.
All sorts of things we heard stories about, and some of them I think we can confirm from our data. Patients would go to their doctor, get their treatments, and rather than risk the uncertainty (or receiving the placebo), they’d put the two together, mix them and divide them by half. We know this, because people who were supposed to be on the placebo already had drug levels in them.’
Much of the pressure came from people with HIV and Aids, and their carers, who wanted the drug released immediately. It was unacceptable to administer a placebo, they argued, if AZT worked. And there was no point having a drug released on the market in 10 years – by that time hundreds of thousands would be dead.
Burroughs Wellcome and many other independent research institutions would spend every subsequent year trying to supplement their data on AZT, trying to find out all the things that would normally be known about a drug before it hit the market. In these later years AZT was to become for many people the symbol of all that was wrong with Aids research. Once AZT was shown to have worked, almost all available funds were channelled to support its development and other potential treatments, along with any doubts that HIV was the cause of Aids, were swept aside.
BUT IN 1986, AZT was unstoppable. It suited the FDA, because it showed the administration was doing something. It suited Wellcome, because it now had a patent on AZT (and by 1986, with the epidemic increasing alarmingly, there was no doubt that the financial rewards would be enormous). It suited doctors, because they believed they could help their patients. And it certainly suited people with Aids. Some people had doubts, but hell, if you were ill and dying you wanted to believe. After all the despair and uncertainty, people in authority were saying ‘take this, it’ll do you good’.
Cottrell was one of the first people to take AZT in Britain. He was prescribed it in 1986, before it was widely available, when he was 23.
‘I had recently been diagnosed HIV-positive, and I went into a panic. I thought I was going to die. I remembered something about this drug coming from America and everyone clamouring to get it. I was perfectly healthy. My boyfriend’s blood count was quite low, and he was prescribed it by St Stephen’s Hospital, and I took it too. Intuitively, I didn’t think it was doing me any good. I was prescribed it three times over a period of three years, and I took it out of fear. I was first prescribed 1,200mg a day, and then 500mg, but I still felt bad, even on the lower dose. I had nausea and headaches and muscle fatigue.’
Cottrell took it every four hours, which meant he had to have a bleeper that woke him at three or four o’clock every morning. (People joked that the real Aids money lay in making these bleepers; in New York in the late Eighties, opera performances were punctuated by bleeps.) Cottrell stopped taking AZT after a few weeks, but then he got scared, and began taking it once more. ‘I got my drugs every two weeks – a big plastic bagful. I felt that I was carrying my life around in that bag.’
His friend, Pierre Hardy, was diagnosed HIV in 1989, when he was 28. At a specialist clinic he was given a sheet of paper which explained that AZT was the most efficient treatment, but also that it hadn’t been around long enough for anyone to know the long-term effects. Like most people in his position, he said he’d try anything, and he was prescribed 500mg a day.
‘My T4 count went up along with my general health in the first year, and everything settled down. I had been on AZT for three years, and my T4 count was levelling between 400 and 600 (an average T4 count in healthy adults is between 800 and 1,000). And then last year I started to get sick. I had repeated chest infections, and in November 1992 I had a stroke. I was hospitalised in a specialist ward. I asked them for my T4 count, and when they came back, they were were uncomfortable about it. My T4 count was 90. I thought I was finished.
‘When I got home and started to review the whole thing, the whole HIV theory. I threw away all the pills I was taking – I was taking seven every morning and evening. I started to change my diet, and then I went back to my doctor. When I had my new T4 count it was 545. I’ve had three migraines since January, a little bit of asthma coming back, but basically I feel much better. If I’d continued to believe in the traditional medicine sytem I would have been dead either this year or next year.’
Two weeks ago Hardy met a volunteer with the Terrence Higgins Trust, who told him that he and his boyfriend were taking AZT and it was working like a dream.
‘I asked him how long they were on it. He said four months. I said that that was the trap that everyone was falling into. The AZT will work for you for a little while, for the maximum of one year, as it did for me, and afterwards the damage became visible.’
Most people with Aids, and many with asymptomatic HIV, take or have taken AZT. Other drugs have emerged in the past few years that work in a similar way – DDC (produced by the Swiss company Hoffmann-La Roche) and DDI (made by the American company Bristol-Myers Squibb), but AZT is still the market leader. It is hard to think of another product that is so dominant in its field. You read the showbiz autobiographies and those three little letters snap out of the page.
Earvin ‘Magic’ Johnson, the basketball star who tested HIV-positive in October 1991, was advised to take AZT immediately. He agreed. ‘There was a lot of public interest in the fact that I was taking AZT, which was originally used only in the later stages of the illness,’ he explained in My Life, his autobiography. ‘These days it’s used as a preventative, but not everybody knew that. That may be why some people, including a few reporters, concluded that I was sicker than I actually was.’ People wrote to Johnson telling him that AZT was not the answer. Somebody advised him to drink all his blood and replace it with new blood. ‘Even now I can’t go anywhere without somebody coming up and saying, ‘I know this friend who knows this doctor who has a cure’.’
Rudolf Nureyev, who died in January, began taking AZT in 1988. ‘AZT was just beginning to be used in France,’ said Michel Canesi, his doctor. ‘I didn’t want to give it to him straight away, because I was worried that the side-effects would hamper him (Nureyev was still dancing at this time). Rudi lost his temper and said: ‘I want this medicine.’ I replied that there hadn’t been long enough to judge the results. But I had to give in and prescribe it – he was so insistent. But he didn’t take it regularly. He went off every time with tons of drugs, and every time I went to see him I found unused packets all over the place.’
The film-maker Derek Jarman, who was diagnosed HIV-positive in 1986, has found AZT beneficial. ‘It works – it holds everything up. It stops the virus replicating. At the beginning they gave people much too massive doses, which affected us physically. I had no recognisable toxic side-effects from it. I began taking it in September 1990, I think, and I came off it last August.
‘I was invited by my doctor to make up my mind whether I took the drug or not, so I rang up various people in America and the general advice was to take it – and this was advice was from quite radical people, not people in with the Wellcome Foundation.
‘I came off it because my doctor said that my (T4) count was down. We’ve never discussed it since. He just suddenly said, ‘I think you’ve had enough AZT, Derek’, and I very much trust him, he’s a brilliant doctor. The whole thing is so complicated, because I took a lot of other drugs as well. I had to have suppressants for TB, toxoplasmosis and PCP. And then obviously if I got an infection there was fluconazole and all of that area. And then at a certain point they added hydrocortisone and fludrocortisone to keep my energy up.’
Jarman has recently been in hospital. ‘At the moment I’m actually on nothing. I’ve had a skin complaint and they decided it would be very sensible to take me off all my pills, and then go back on the drugs to see if they were causing the skin complaint. They can obviously play around with the drugs.
‘My feeling about AZT is that I’m glad I took it, even though I can’t prove to you that it did anything. You can say that if it helps someone psychologically then it must be doing some good. I think the doctors generally feel that it does some good. But how do you know?’
FINANCIALLY, Wellcome plc has done extremely well out of AZT. Retrovir, the drug’s brand name, accounts for more than 13 per cent of its total income, and yielded pounds 213m last year. As the only big earner to have been launched by the company in the past decade, the continued success of AZT is crucial to its growth. The company will be well aware that at the end of last year the World Health Organisation estimated that about 13 million men, women and children have been infected with HIV since the start of the pandemic. (A large proportion of these cases are in sub-Saharan Africa and South and South-east Asia, where AZT and other anti-Aids treatments are unlikely to be available or affordable; the figure for HIV infection in the Americas and Western Europe is estimated at 2.5 million.)
Part of the Wellcome Foundation was floated on the stock market in 1986, the year of the AZT breakthrough. Subsequent rises in share prices have been directly linked to the fortunes of the drug and the results of new trials. In February 1987, the share price jumped 73.5p to 374.5p on the news that AZT would be widely available in the US at dollars 188 for 100 capsules, an extremely high price for a new drug, and one that would yield large profits (this translated to about dollars 10,000 a year for every user). By November 1989 the share price had almost doubled to 724p; year-on-year pre-tax profits were up 28 per cent to pounds 283m. In early 1993, the share price was at 810p; last year’s pre-tax profits were pounds 505m.
‘In terms of the emotive quality of the demand, there’s never been a drug like it,’ said Martin Sherwood, a Wellcome spokesman, shortly after AZT’s launch. It was just this emotive demand that led to the picketing of the Wellcome shareholders’ meeting in January 1990. Act Up (the Aids Coalition to Unleash Power, co-founded by the playwright Larry Kramer) picketed the AGM at Grosvenor House in London, describing it as ‘a gathering of Aids profiteers’. Activists complained about the price of AZT, and what they saw as Wellcome’s reluctance to provide all available information on the drug.
Wellcome shareholders were irritated by this intrusion, not least when Act Up members interrupted the meeting and insisted on talking to Sir Alfred Shepperd, the outgoing chairman. But Wellcome executives were baffled: they believed they had done everything they could to benefit people with HIV and Aids, certainly more than any other pharmaceuticals company. Was it not these very same activists who had celebrated when AZT was launched three years earlier? At first Wellcome defended its pricing on the grounds that AZT took dollars 80m to develop and produce (later revised to dollars 30m), but it soon bowed to pressure (and its economies of scale) and cut the price. The recommended dosage was also reduced for medical reasons, which meant many more people could tolerate its toxicity. Today AZT costs about dollars 3,000 per person per year, or about pounds 2,000.
As would be expected, Wellcome plays up the good news. When, in 1989, two double- blind placebo trials of the effects of AZT on asymptomatic and less seriously ill patients showed that it could delay the progression of the disease, much was made of the results and the share price rose by 30p. But when, four months later, the company admitted that AZT had caused cancer in rodents, it explained that the rats and mice were given 10 times the dose prescribed to humans, and that several other drugs in use by humans had also produced tumours in animals when administered over long periods. Wellcome’s share price went down one penny.
Wellcome’s PR machine is an impressive force, and much money is spent on convincing the media of AZT’s worth. You go and see them and you get a lot of bumph: how AZT works, why it is more effective than other anti- retrovirals. Wellcome house-magazines talk of the extra 400,000 productive years of life it has made possible through the drug, about how many thorough and independent studies have stressed AZT’s efficacy.
‘The number of people who have shown agression against us concerns us no end,’ says Trevor Jones. ‘Normally the company tries to distance itself from the patient / physician interaction – it must do. The day-to-day therapy of the patient is not our responsibility. But about three years ago we started to open our labs to people with HIV and their carers, contrary to the advice of my security and other colleagues. You then realise the uncertainty and the frustrations involved in that act of taking a tablet for the very first time. When people with HIV came through the door of the lab I could almost touch their anger. But I realised that the anger was not really about Wellcome or me, but about their mortality. They were frustrated, and saying, ‘Please, please what can I do?’ These were genuine cris de coeur.’
Dr Jones is one of the few pharmaceutical industry representatives on Britain’s Medical Controls Agency. Wellcome has clearly selected its spokesman with care. ‘People say we’re purely acting out of commercial interests, but it is not in our commercial interests to do anything else but get this drug right,’ Dr Jones says. ‘We wanted to show people that we are working night and day, weekdays and weekends trying to develop better medicines. Otherwise we look like ogres and robber barons all the time. That’s the whole history of our business; if you’ve got a problem with a product, you must, you must, you must tell people. The criticism hurts a lot; our integrity as a scientific body is important to us. I don’t take too kindly to people saying, ‘Oh, you don’t want to listen to Wellcome, because they would say that, wouldn’t they?’ You can’t hide anything in this business, because otherwise who will trust us when we develop another drug, like the new epilepsy drug we’ve got now? You have to believe that the integrity of science is good.’
Jones has had a bad few weeks. Wellcome’s share price was hammered by last month’s Concorde trial report, falling 10 per cent to 670p, before rallying to 692p. Five days after the report appeared, Wellcome staged a damage limitation exercise, at which Jones told a press conference that he was unhappy with the way the results were released, without peer review or advice to patients, and saying it had caused panic among those with HIV. He said that the full results had yet to be released, and hoped that a more beneficial picture of early intervention with AZT would emerge at the ninth International Aids Conference in Berlin in June. He also outlined that the protocol of the study had changed from that agreed in 1988. When an American study reported in 1989 that AZT did have beneficial effects on people with asymptomatic HIV, the Concorde officials decided that people on its trial could switch to AZT if they wanted to; this may have led to a diluting of the results.
Last week, Jones reiterated why AZT may still be beneficial, and why doctors should continue to prescribe the drug early. ‘We have gathered together 10 studies on asymptomatic patients. Five of these are control studies with placebos, and five are cohort studies, in which we simply give the drug and observe what happens. These studies involved more than 6,500 patients and ranged from one to four years in duration. We believe we have accrued sufficient data to show that taking the drug when you’re asymptomatic does delay the onset of further symptoms.’
WELLCOME has a presence at all the chief Aids conferences, and will occasionally organise gatherings of its own. In June 1992 it launched Positive Action, ‘an international intiative’ in support of those with HIV and Aids. For the launch conference in London, journalists flew in from all over Europe to hear Wellcome executives describe how pounds 1m was being distributed to many educational organisations. An emotional climax of sorts was provided by Jerry Breitman, the company’s US director of professional relations. He was there to present the ‘workplace initiative’, and his speech contained a little surprise at the end. Like the wig salesman whose coup de grace is to rip off his own toupee, Breitman declared himself HIV-positive. ‘I thought long and hard before deciding to tell my management,’ he revealed. ‘But . . . when you are part of an enlightened organisation such as Wellcome, I am absolutely convinced that communicating your HIV infection is a positive action . . . It is, truly, one of the best decisions I have made in a very long time.’ A few journalists felt distinctly queasy at the theatricality of it all.
One of the initiatives raised was Wellcome’s involvement with the Terrence Higgins Trust. This first surfaced in 1991, with the publication of four information leaflets. Two months ago staff at the Trust and volunteers read in their newsletter that the link had been strengthened. The newsletter explained that ‘THT, along with the Wellcome Foundation, is about to begin producing an important new medical information series. THT are providing a series of medical updates for all staff and volunteers. We will be providing them on a regular basis every two months in the evening. Costs will be met by the Wellcome Foundation, which also funds our series of general booklets.’
Nick Partridge, chief executive of the trust, is dubbed ‘Nick the Sick’ on the placards carried by the protesters outside his office. Partridge, in reply, calls them ‘New Age flat- earthers who have a naive hope that Holland & Barrett will produce a herbal tea that will be effective against HIV.’ Partridge said that the trust actively pursued funding from a wide range of companies and government agencies, and that it was ‘quite clear that none of that funding involves an ability by those companies to influence the information we produce. We would be neglecting our duty if we were not in regular contact with Wellcome, Bristol-Myers Squibb and Roche, arguing for greater investment in HIV research and fair and balanced information. The leaflets are not about treatment issues.’
But once they were. In 1991 the trust produced a 24-page booklet on HIV and its treatment; nine pages were devoted to AZT, but only half a page was given to other therapies. The copyright on the leaflet was held by the Wellcome Foundation, which also paid for its printing. ‘It was only available for eight months,’ Partridge says. ‘Information changes quite rapidly. The main fault of that leaflet is that it is too hopeful. By 1991 the hopes around early intervention had probably gone further than we realise, in retrospect, was wise. The desire by many people with HIV to say, ‘Yes, we can live with this infection’ meant that a lot of hope was invested in the theory of early intervention. For all its faults, our leaflet was still a lot more realistic than the material that Wellcome was putting out on its own. Remember that over the years, there have been many stories of breakthroughs that proved to be wildly optimistic.’
FOR MOST people with HIV, the AZT dream is over. AZT is the future that was; no one believes in the ‘magic bullet’ any more. It does have benefits for some patients who are seriously ill, but there is now severe doubt over its other uses. This, after the drug has been subjected to more tests, and has been the subject of more post-launch research papers, than perhaps any other modern therapy.
The future for HIV and Aids treatment appears to be in combination treatment – the use of AZT and DDC and DDI and many other compounds used in all manner of variations. Several trials are in progress. Two weeks ago it was announced that Wellcome has joined forces with its competitors Hoffman-La Roche, Bristol-Myers Squibb, Glaxo, SmithKline Beecham and 15 other companies, in an attempt to pool their research knowledge and find an effective treatment.
Wellcome is also developing some other anti-Aids drugs on its own. We won’t hear about these for a while; the company doesn’t want to raise any hopes.
Jerome Horwitz, the man who created AZT in 1964, is still active in medical research. He’s 74 now, but you can still reach him most days at the Meyer L Prentis Cancer Center in Detroit. Occasionally he does a little Aids work, but most of his time involves cancer chemotherapy.
Horwitz believes AZT is not the answer to HIV and Aids, but has hopes for combination therapies (he was also the first to synthesise DDC). He concludes that AZT ‘buys time’.
‘We were certainly on the cutting edge,’ he says of his work in the mid-Sixties. ‘When the pharmacologist said, ‘Look, Dr Horwitz, your compounds are not effective against leukaemias and I see no future for them’, that was like a blow to the solar plexus. We had great hopes. ‘I remember one of my students saying at the time that we had a great series ofcompounds just waiting for a disease totreat. It took 25 years before our beliefs were vindicated.’
The first Horwitz heard of AZT’s use against HIV was when he read about it in the Wall Street Journal. Burroughs Wellcome established a chair in his name at the Michigan Cancer Foundation, but he has received no financial reward.
‘My wife sits across from me at the
breakfast table and reminds me of all the
money that Burroughs Wellcome has got out of it and I haven’t got a dime. I keep telling her about the legacy I’m leaving. But I wouldn’t be being absolutely straight with you if I hadn’t thought that I should have gotten something out of it.’-
For years, Rosemary Kennedy’s story was kept secret after her lobotomy was botched, leaving her unable to walk or talk.
The Kennedy Family at Hyannis Port on September 4, 1931. From left to right: Robert, John, Eunice, Jean (on lap of) Joseph Sr., Rose (behind) Patricia, Kathleen, Joseph Jr. (behind) Rosemary. Dog in foreground is “Buddy.”
Though John F. Kennedy and Jackie might be the most recognizable members of the family, the Kennedys were famous long before John became president.
Their father, Joe Kennedy Sr., was a prominent businessman in Boston and his wife, Rose, was a noted philanthropist and socialite. Together they had nine children, three of whom went into politics. For the most part they lived their lives in the open, almost like America’s version of a royal family.
But, like every family, they had their secrets.
Born in 1918, Rosemary Kennedy was the third child of Joe and Rose and the first girl. During her birth, the obstetrician who was supposed to be delivering her was running late. Not wanting to deliver the baby without a doctor present, the nurse reached up into Rose’s birth canal and held the baby in place.
The actions of the nurse would have lasting consequences for Rosemary Kennedy. The lack of oxygen delivered to her brain during her birth caused lasting damage to her brain, resulting in a mental deficiency.
Though she looked like the rest of the Kennedys, with bright eyes and dark hair, her parents knew she was different right away.
As a child, Rosemary was unable to keep up with her siblings, who would often play ball in the yard, or run around the neighborhood. Her lack of inclusion often caused “fits,” which were later discovered to be seizures or episodes relating to her mental illness.
However, in the 1920s mental illness was highly stigmatized. Fearing repercussions if her daughter couldn’t keep up, Rose pulled Rosemary out of school and instead hired a tutor to teach the girl from home. Eventually, she sent her to a boarding school, in lieu of institutionalizing her.
In 1928, Joe was named an ambassador to the Court of St. James in England. The entire family moved across the Atlantic and was presented at court to the public. Despite her disabilities, Rosemary joined the family for the presentation.
Of course, no one knew the extent of her disability, as the Kennedys had worked hard to keep it quiet.
Keystone/Getty Images Rosemary, her sister Kathleen, and her mother Rose being presented to the people in London. Her family abandoned her and kept her shuttered away in institutions for the rest of her life.
In England, Rosemary gained a sense of normalcy, as she had been placed in a Catholic school run by nuns. With the time and patience to teach her, they were training her to be a teacher’s aide and she was flourishing under their guidance.
However, in 1940, when Germany marched on Paris, the Kennedys were forced back to the states, and Rosemary’s education was abandoned. Once back stateside, Rose placed Rosemary in a convent, though it didn’t last long. According to the nuns, Rosemary would sneak out at night and go to bars, meet strange men and go home with them.
At the same time, Joe was grooming his two oldest boys for a career in politics. Rose and Joe worried that Rosemary’s behavior could create a bad reputation not just for herself but for the whole family, and eagerly searched for something that would help her.
Dr. Walter Freeman was the answer.
Freeman, along with his associate Dr. James Watts had been researching a neurological procedure that was said to cure the physically and mentally disabled. The procedure? The lobotomy.
When it was first introduced, the lobotomy was hailed as a cure-all and was widely recommended by physicians. Despite the excitement, however, there were many warnings that the lobotomy, though occasionally effective, was also destructive. One woman described her daughter, a recipient, as being the same person on the outside, but like a new human on the inside.
John F. Kennedy Presidential Library and Museum The Kennedy family, not including baby Jean.
Despite the warnings, Joe needed no convincing, as it seemed like this was the Kennedy family’s last hope. Years later, Rose would claim that she had no knowledge of the procedure until it had already happened. No one thought to ask if Rosemary had any thoughts of her own.
In 1941, when she was 23 years old, Rosemary Kennedy received a lobotomy. Two holes were drilled in her skull, through which small metal spatulas were inserted. The spatulas were used to sever the link between the pre-frontal cortex and the rest of the brain. Though it is not known whether he did so on Rosemary, Dr. Freeman would often insert an icepick through the patient’s eye to sever the link as well as the spatula.
Throughout the entire procedure, Rosemary was awake, speaking with doctors and reciting poems to nurses. They knew the procedure was over when she stopped speaking.
Immediately after the procedure, the Kennedys realized that something was wrong.
John F. Kennedy Presidential Library and Museum John and his siblings Eunice, Joseph Jr., Rosemary, and Kathleen in a boat at Cohasset, Massachusetts, circa 1923-1924.
Rosemary could no longer speak or walk. She was moved to an institution and spent months in physical therapy before she regained movement, and even then it was only partially in one arm.
Rosemary Kennedy spent 20 years in the institution, unable to speak, walk, or see her family. It wasn’t until after Joe suffered a massive stroke that Rose went to go see her daughter again. In a panicked rage, Rosemary attacked her mother, unable to express herself any other way.
At that point, the Kennedys realized what they had done and began to champion rights for the mentally disabled.
John F. Kennedy would use his presidency to sign the Maternal and Child Health and Mental Retardation Planning Amendment to the Social Security Act, the precursor to the Americans with Disabilities Act, which his brother Ted pushed for during his time as a senator. Eunice Kennedy, JFK and Rosemary’s sister also founded the Special Olympics in 1962, to champion the achievements and abilities of the physically and mentally disabled.
After being reunited with her family, Rosemary Kennedy lived out the rest of her life in Saint Coletta’s, a residential care facility in Jefferson, Wisconsin, until her death in 2005.
Photo Illustration by Lyne Lucien/The Daily Beast/Getty
In 1942, the exposure of a Brooklyn townhouse where wealthy men had sex with members of the armed services led to an anti-gay witch-hunt and heated political scandal.
n the early part of the 20th century, brothels were commonplace in many neighborhoods in New York City, but in 1942 an inconspicuous two-story redbrick town house at 329 Pacific Street—a run-down block near the border between Brooklyn Heights and downtown Brooklyn—would become the most famous “house of assignation” in the entire country.
The proprietor, a fifty-five-year-old, “moon-faced” Swedish immigrant, Gustave Beekman, specialized in providing wealthy men with members of the armed services.
He had previously run a similar house a few blocks closer to the water at 235 Warren Street, but had relocated after being busted in a police raid in November 1940. At that time, he was charged with running a disorderly house, fined, and quickly released.
However, when the police raided his establishment on Pacific Street on the evening of March 14, 1942 (accompanied by members of the Office of Naval Intelligence), they would uncover a scandal that would rock the nation, consume newspaper headlines for months, and get hotly debated on the floor of the US Senate.
Or perhaps it’s more accurate to say they would invent one. It would be Walter Winchell, then the gossip columnist for the New York Daily Mirror, who would give this strange episode in Brooklyn history its enduring name: “The Swastika Swishery.”
This was one of the stories I’d heard about early in my research for my new book, When Brooklyn Was Queer, but I never suspected that I would uncover new information that would answer many of the lingering questions about this so-called scandal.
The initial story, which was primarily reported in the New York Post, went something like this: Beekman ran a “house of degradation” where German spies hired American servicemen to pump them over pillow talk for information about troop movements.
From there, the story quickly spiraled. Not only were there spies at Beekman’s house, a notorious “Senator X,” who was well known as a closeted gay man and opposed America’s entry into World War II, was also a regular habitué of Beekman’s. By early May, Beekman wasn’t just accused of hosting any old spy; rather, he was catering to “one of Hitler’s chief espionage agents in this country.”
For all of April and May, papers kept readers riveted with headlines such as “Service Men Lured to ‘Den’ Called Spy Nest,” “Senator Linked to Spy Nest Which Lured Service Men,” “Den Keeper Withholds Source of Cash,” and “Leibowitz Pushes Spy Ring Probe: Tells Convicted Morals Offender to Talk or Get 20-Year Term.”
News bulletins eagerly broadcast every new tidbit of information in the case, including the four separate (and contradictory) official statements Beekman gave to the police and the FBI.
The senator in question was soon revealed as David Ignatius Walsh, a Catholic “confirmed bachelor” from Boston, who—although liberal on many social issues—was a strong isolationist, believing America had no place in the affairs of Europe.
Time magazine called his connection with the Beekman case “one of the worst scandals that ever affected a member of the Senate.” When the Senate majority leader opened discussion of the issue on the Senate floor, he called the FBI’s report on the case “disgusting and unprintable” and refused to have it entered into the Senate’s official record.
“To this day, numerous authors have speculated about what actually happened at Beekman’s house in the middle of World War II, with most concluding that it was ultimately unknowable”
Another isolationist senator from Missouri called Dorothy Schiff, the publisher of the New York Post, an “old hussy” and demanded an investigation on the charge that she was part of a secret cabal that was trying to gin up public sentiment in favor of the war by making antiwar politicians look bad.
To this day, numerous authors have speculated about what actually happened at Beekman’s house in the middle of World War II, with most concluding that it was ultimately unknowable.
However, Dorothy Schiff was so concerned that Senator Walsh might sue the Post over its reporting that she secretly commissioned a team of six private investigators and attorneys, led by Daniel A. Doran, to discover the truth.
Their report, which took five months to prepare, ran over 150 pages and included everything from interviews with the major players in the case (including Beekman and all of his lawyers), to a detailed analysis of Senator Walsh’s travel schedule for the times he was supposedly in Brooklyn.
For years, this report has been publicly available, along with the rest of Dorothy Schiff’s papers, at the New York Public Library, but no historians seem to have referenced it. As far as I know, I am the first to read its findings.
Local police had had Beekman under watch at least as far back as January 1942, having noticed an unusual number of sailors and soldiers coming and going from his building. In the two years since they had last busted Beekman, the war had begun, and no one wanted to arrest a bunch of men who might be needed in Europe or to impugn the morality of the military in general.
The police had no plans to raid his house until they were contacted by the Office of Naval Intelligence (ONI), which had secretly set up a spy post on the fourth floor of a nearby hospital, from which they were recording the license plate numbers of everyone who entered the building.
The ONI wasn’t interested in Beekman; rather, it was trailing William Elberfeld, a German national whom it believed to be a spy for Hitler. Together, the police and the ONI raided the establishment, arresting not just Beekman, but some of his clients (including noted composer Virgil Thomson), and some of the men who worked there.
“The prosecution seemed convinced that Beekman couldn’t be making much money from running a house of male prostitution, and so he had to have some other source of income—perhaps from Elberfeld or another spy”
One of the sex workers arrested was a Brooklyn merchant mariner named Charles Zuber, who was also one of Beekman’s lovers.
The assistant district attorney (ADA) on the case, eager, perhaps, to make a name for himself, questioned Zuber at length about any particularly wealthy clients. The prosecution seemed convinced that Beekman couldn’t be making much money from running a house of male prostitution, and so he had to have some other source of income—perhaps from Elberfeld or another spy.
Zuber furnished the ADA with the name “Walsh,” saying he believed the man to be a doctor. The ADA, aware of the long-standing rumors that Senator David Walsh was gay, jumped to the conclusion that these two men were one and the same. He offered Zuber a deal: if he flipped on Beekman and testified against him on sodomy charges, Zuber would get off scot-free.
The ADA then passed the information about Walsh on to the judge in the case. When Beekman was found guilty on charges of sodomy, largely thanks to Zuber’s testimony, the judge told Beekman that if he came clean about the extent of the spy ring, he would be lenient; otherwise, Beekman was facing a twenty-year sentence.
“He seemed willing to say whatever was necessary to avoid going to prison, which for a fifty-five-year-old gay man whom the nation now believed to be a Nazi sympathizer might well have been a death sentence”
According to the lead investigator hired by Dorothy Schiff, Beekman was “ingratiating, well-mannered, well spoken and plausible.” He was also terrified and rather loose with the truth. He seemed willing to say whatever was necessary to avoid going to prison, which for a 55-year-old gay man whom the nation now believed to be a Nazi sympathizer might well have been a death sentence.
Elberfeld had been a regular at Beekman’s place, but he also ran a rival brothel in Manhattan and had no need to go to Brooklyn if he wanted to question sailors. Moreover, Beekman had banned him from his house around Thanksgiving of 1941, when Elberfeld told Beekman that Sweden was next on Hitler’s list, and that after it was invaded, Beekman wouldn’t be so “uppity-uppity.”
The police literally tore apart both Beekman’s home and Elberfeld’s apartment and found nothing except a shortwave radio at Elberfeld’s, which was technically contraband when owned by a foreign national.
Elberfeld was placed on indefinite detention on Ellis Island—where he would remain for the rest of the war—but no charges were ever brought against him, and the police and the ONI no longer seemed interested in him at all. Instead, they leaned on Beekman to identify Walsh, once grilling him for over seven hours until he collapsed.
A few of the men arrested in the initial raid were also asked about Walsh, with some saying he was there, others saying he wasn’t, and a few saying they had no idea.
With no evidence other than a series of contradictory statements on whether Walsh had ever been at Beekman’s home, there was no case. Yet the government still believed that Beekman was hiding some source of income, which the judge seemed to believe would have linked Walsh to the story.
When Beekman refused to name his (nonexistent) financial backers, he received a twenty-year sentence to Sing Sing, the maximum-security prison in Ossining, New York.
By making a detailed analysis of Walsh’s travel schedule, investigator Doran conclusively proved that Walsh could not have been at Beekman’s establishment on any of the dates he was supposed to have been present.
“No one seemed interested in using that evidence to exonerate Beekman, who would serve out the entirety of his twenty-year sentence before emerging from prison (where he was called ‘Mother Beekman’) and disappearing from public records entirely”
Moreover, Doran tracked down a Connecticut doctor, Harry Stone, a regular at Beekman’s who bore a distinct resemblance to Senator Walsh. By presenting photos of Walsh and Stone to various witnesses (including Beekman), Doran concluded that Stone was almost definitely the man mistaken for Walsh.
Yet no one seemed interested in using that evidence to exonerate Beekman, who would serve out the entirety of his twenty-year sentence before emerging from prison (where he was called “Mother Beekman”) and disappearing from public records entirely.
As for Walsh, although his fellow Senate members congratulated him on his aplomb during the entire affair, the airing of his gay laundry (plus, no doubt, his opposition to the war) seemed to sour voters on him. He was ousted from the Senate in 1946 and died the next year.
After months of wild accusations, sting operations, and endless denunciations to the press, all the government got was the pointless destruction of the lives of two gay men and a witch hunt that sent innumerable others into hiding.
Today, the quiet red-brick building still sits at 329 Pacific Street as a private residence, with no trace of its infamous past showing in its innocuous façade.
Decades before gay marriage became legal anywhere in the US, same-sex couples were committing themselves to each other in front of friends and loved ones. Few records of these ceremonies existed – until now, writes Jonathan Berr.
In 1957, a man dropped off a roll of film at a pharmacy in Philadelphia. But the developed photos were never returned to their owners.
The pictures appear to depict a gay wedding, nearly 50 years before same-sex marriage was legal anywhere in the US and almost 60 years before it became a federally-recognised right.
Now, a trio of gay producers and writers are trying to identify the grooms to learn their story and to find out whether a pharmacy employee balked at providing the snaps because they objected to their subject.
The writers are documenting their efforts in a reality show The Mystery of the 1957 Gay Wedding Photos.
The programme, which doesn’t yet have a platform to call home, is being produced in conjunction with Endemol Shine Group, whose shows include Big Brother, The Biggest Loser and Extreme Makeover: Home Edition.
ONE Archives at USC
“It’s a passion project for us,” says Michael J. Wolfe, a Los Angeles-based writer. “We are turning over every stone, interviewing dozens of people in the Philadelphia area and beyond, and consulting with investigators, historians, and experts across many different fields.”
The photos were acquired by a collector a few years ago who had bought them at an online auction. He realised their significance and donated them to ONE Archives at the USC Libraries in Los Angeles and at the Wilcox Archives in Philadelphia.
The couple in the pictures appear to be in their 20s or 30s, so they would be in their 80s or 90s if they were alive today. The grooms and their guests are dressed up in dark suits with flowers in their lapels.
The celebration took place in a modest flat with the blinds drawn. It featured a ceremony officiated by someone who appears to be a member of the clergy. The grooms are shown kissing, cutting their wedding cake and opening presents.
ONE Archives at USC
Mr Wolfe and his partners, filmmaker PJ Palmer and TV writer/producer Neal Baer, have not identified the mystery couple yet.
“We are recovering amazing, important stories all sorts of them… and more gay history that’s been buried,” he says.
“There is a very rich history that’s been suppressed… I wish as a child [that] I had seen family photos of a marriage like this… I would have felt more normal as a kid. I would have known that I was okay.”
Couples who fell in love sometimes committed themselves to one another in unions that were not acknowledged by either governments or religions.
The US Supreme Court didn’t recognise the right for gay people to marry the person of their choice until 2015, 11 years after Massachusetts did so.
ONE Archives at USC
“We don’t know how common or uncommon it was for couples to hold ceremonies to marry each other [because] there is so little photographic or film record of how people actually lived,” says Eric Marcus, host of the Making Gay History podcast.
“It’s important to remember that people found ways to live their lives quietly away from the prying eyes of the straight world.”
Of course, that was easier said than done.
Wedding guests at the mystery wedding ONE Archives at USC
Several years before the wedding took place, President Dwight Eisenhower signed an executive order banning gays from working for the federal government.
In 1952, The American Psychiatric Association classified homosexuality as a “sociopathic personality disturbance” in the first edition of its Diagnostic and Statistical Manual (DSM), the listing of known psychiatric disorders.
After considerable lobbying by activists, the APA removed homosexuality from the second edition of the DSM in 1973.
The Stonewall Riots, considered to be the birth of the modern gay rights movement, had happened a few years before that in 1969 – 12 years after the wedding.
ONE Archives at USC
It’s not just the passage of time that will hinder the search for the grooms. The filmmakers believe the Aids crisis may also be factor – about 700,000 Americans have died since the start of the epidemic in the 1980s, according to the Kaiser Family Foundation.
“We are talking about a generation of people who were decimated by Aids,” Mr Wolfe said. “There are a lot of missing people who otherwise would have made a search like this much easier. All of that happened before social media.”
If the couple is ever identified, they would certainly add another chapter in the history of gay rights for doing something extraordinary that is now becoming increasingly ordinary.