Corsets became popular in the 16th century allegedly because Catherine de’ Medici, wife of French King Henry II, banned women with thick waists from attending court. She was a tyrannical monarch, but the Italian-born woman created beauty standards that held up exceptionally well. Corsets remained incredibly common during the Renaissance, up until the 20th century. Certain historians, however, suggested the restrictive undergarments contributed to the patriarchal system of female oppression.
The inherent tightness of the shapewear appealed to the male-dictated understanding of femininity and attractiveness. So unsurprisingly, women wore corsets to their own detriment. They suffered to achieve a smaller, more socially acceptable waist. Many 21st century beauty trends are as focused on the hourglass shape as well, but there are so many things people don’t know about corsets.
Napoleon Claimed Corsets Contributed To The Decline Of Humanity
Napoleon Bonaparte not only quested to rule Europe, he also campaigned to do away with corsets. The dictator called the shaping undergarment “the implement of detestable coquetry which not only betrays a frivolous bent but forecasts the decline of humanity.” And while Bonaparte’s female lovers still wore corsets, less hypocritical medical professionals believed the clothing could cause infertility. In fact, C.J. Dickinson, professor emeritus at Wolfson Institute of Preventive Medicine, says that extremely tight clothing may result in endometriosis, causing lesions on the uterus lining. When constricted, these lesions can’t shed during menstruation; internal bleeding may occur, and scar tissue might form.
Women were not the only aristocrats wearing corsets to create more socially acceptable figures. Specifically, in the latter part of the 18th century men wore form-fitting trousers and jackets. Corsets helped gentlemen achieve a smoother silhouette. However, French and Englishmen grew tired of the trend by the middle of the 19th century. Those who continued to wear the undergarments were teased.
Austrian men continued to wear corsets despite changing fashion standards in the rest of Europe, though. One English gentleman who attended an elite Austrian boarding school noted in the 1867 issue of The Englishwoman’s Domestic Magazine:
From personal experience, I beg to express a decided and unqualified approval of corsets. I was early sent to school in Austria where lacing was not considered ridiculous in a gentleman as in England, and I objected in the thoroughly English way. A sturdy [school attendant] was deaf to my remonstrance, and speedily laced me up tightly in a fashionable Viennese corset… It is from no feeling of vanity that I have ever since continued to wear them fro, not caring to incur ridicule, I take good care that my dress shall not betray me…
Corsets date back at least as early as the 16th century. Aristocratic women started to wear bodices reinforced with whale bones and tusks, instead of the original ones made from cloth and silk. Eventually, pieces of wood and metal were added to the front of most corsets to create even more structure. Duchess of Montpeniser Anne Marie Louise d’Orléans actually had a predominantly metal corset decorated with a crown and fleur-de-lis.
Some 19th-Century Medical Professionals Discouraged Tightly Laced Corsets
Not all citizens condoned corsets or the tight lacing that became popular once metal eyelets were added to the undergarments. In fact, Lancet, one of the oldest medical journals, produced a few articles about the dangers of corsets in the 1880s and ’90s. Additionally, The Sacred Heart Review mentioned in 1890:
Tight lacing] cannot be but hurtful… the veriest novice in anatomy understands how by this process almost every important organ is subjected to cramping pressure, its functions interfered with, and its relations to other structures so altered as to render it, even if it were itself competent, a positive source of danger to them.
Moreover, surgeon William Henry Flowers wrote in his 1881 book, Fashion in Deformity, that tightly-laced corsets were just as harmful as skull-shaping and foot-binding.
Women wore corsets for centuries, but when metal eyelets were added to the undergarments in the 1820s and 1830s, tight-lacing became incredibly popular. This trend involved threading the strings of the corset through the eyelets and pulling considerably. Women were able to be tied in without concern of reverting back to their natural forms. This tight-lacing allegedly caused young women to faint, though; their breathing was constricted. When ladies passed out from lack of oxygen, acquaintances loosened their corset laces or stays. Air then flowed more freely into the lungs. Certain analysts believe excessively tight clothing results in heartburn, distension, and varicose veins because of restricted blood flow.
Not All Corsets Were Used To Make The Waist Appear Slimmer
European corsets in the beginning of the 16th century created an exceedingly recognizable form. An aristocratic woman’s bosom was pushed upward when she wore the shaping garment; her upper half appeared fuller. The torso was shaped like a cylinder because of an unyielding material that ran down the front of the corset. The shaping devices looked more like cones in the 17th century, though. Two pieces of fabric with thick boning were combined to make the waist seem even more narrow.
From about 1800 to 1830, corsets were more forgiving. Women’s stomachs were left unbridled. The undergarments were smaller and more like 21st century bras.
Corsets Changed Shape As Different Monarchs Took The Crown
The Victorian era began when Queen Victoria took the crown in 1837. Corsets during her reign, once again, restricted the belly. Hourglass figures were incredibly popular, so even longer restrictive undergarments were necessary, extending past the natural waist. Steel boning helped create the shape. To make ladies appear appear more shapely, Victorian fashion called for tops with large shoulders and hoop skirts covering multiple layers of crinoline. Clothing designers also began to mass-produce corsets during the Industrial Revolution; people were able to access them more easily.
When Queen Victoria died in 1901, the style changed again. King Edward’s courtiers wore corsets with an “S-bend.” These undergarments typically forced women to tilt forward; their hips and bosom pushed forward, while their backs had an unnatural dip.
Women Who Wore Them Were More Susceptible To Tuberculosis & Pneumonia
Corsets didn’t only cause fainting spells. They also tightly restricted female wearers’ lungs. The vital organs weren’t able to fully expand, making breathing painful. Deep breathing was almost impossible. Additionally, lung conditions, like tuberculosis and pneumonia, could be exacerbated by the corset. Women were especially susceptible to these illnesses before vaccines were invented in the 20th century because their lower lungs were almost constantly bound.
They Caused Back Problems & Women Increasingly Relied On Them
Women who wore corsets for an extended period of time often experienced painful back problems. The boning in the undergarments was mostly immobile; posture remained straight as long as the corsets were laced. This rigidity sometimes led to back and pectoral muscle atrophy, though. The tissue just wasted away. As a result, some corset wearers were forced to rely on their corsets to stay upright.
Women May Have Started Wearing Them As Early As 2000 BCE
In the late 19th century, British archaeologist Sir Arthur Evans discovered a Cretan figure dating back to about 2000 BCE. The sculpture depicted a topless woman with an extremely small waist that looked to be cinched by a belt. Ancient Greeks also wrote about women’s undergarments which made waists tiny and perhaps flattened the bosom.
Fashion trends change frequently. And by the 1920s, nobody wanted to wear corsets anymore. Flapper dresses came into style. The more forgiving clothing gave wearers a more androgynous look. An hourglass figure was no longer the epitome of feminine beauty. The women who wore these flowing garments were usually young and single. Many of them held jobs during the day and partied at night. In addition to removing their corsets, flappers also chopped off the long locks that were characteristic of Victorian women.
In 1999, both “Blue” magazine (the “Bucking the Condomocracy” article, also reprinted in “Out” Magazine, July 1999, Vol. 7, No.12), and “HQ” magazine (“They Shoot Barebackers Don’t They?”) published articles on barebacking, the one in “HQ” being a reprint of an article from “Poz” magazine. The latter caused a bit of a furore in both “The Sydney Star Observer”, and in the “Sydney Morning Herald”…probably understandably. Read in the context of HIV education and safe sex messages at that time, they read almost as a promotion of barebacking.
I was writing regularly for “Talkabout” magazine at the time, and was on the magazines working group. When I read both articles, I thought they elicited a response, and started to put an article about it together. However, several things were going on at “Talkabout”’ at that time, most notably was a new editor, and I was unsure of how liberal she was going to allow the writing to be, and secondly was an article I had written about the “Options” Employment Agency, which was operating on Oxford St at the time, supposedly to assist HIV/AIDS people to return to work after surviving AIDS, or to re-educate. I had written an expose of them not really doing much to actually assist people, and using said clients to do unpaid “work experience” in their offices. The editor, in all fairness, had sent the article to them… and their response was to threaten to sue the organisation (PLWHA NSW), the magazine, and myself. It was “Bring it on!” from my perspective, but obviously from the organisations…and funding…perspective, it wasn’t something they wanted..As it turned out, my accusations were accurate (I had been quite outspoken about what was going on there for some time,…and had the written testimony of a number of guys who had personally encountered the rort…and had even had the office manager of Options…whose name escapes me now…invite me into his office, and made veiled threats about what I was saying) and the agency had its funding stopped, and closed down shortly after. The article was published, but was so heavily edited that it lost all its clout. I was very disappointed.
However, this made me a bit dubious about publishing another controversial article, and being unsure about the editors response to this piece, and time then passing, I never completed the article. I have been republishing most of my “Talkabout” articles on my blog over the last couple of years…some re-edited, some not…and came across the original draft for this article. I couldn’t actually remember the content of the magazine articles, so did a bit of googling, and thanking the gods of cyberspace that nothing ever disappears completely in the ethos…I found both original articles. I will now include them in my article, to have a permanent record of them. They both make interesting reading.
About 18 months or so further down the line, and with a different editor, I wrote yet another controversial piece on bug chasing…heavily researched, so unbiased…that was totally pulled from publication by the then “Talkabout” working group. It was with great trepidation that Glenn, the then editor, rang to tell me the decision. He knew how much work had gone into it, and I cannot ever recollect an article, written by a HIV+ man, being pulled from publication before in “Talkabout”. The reasoning: it was a great article, but because “Talkabout” was funded by NSW Community Health, there was a perception that said organisation may have seen it as a “promotion of the act of bug chasing” rather than an expose. I was furious. Bug chasing was being talked about within the HIV community, the whole sex dating mentality of “breed me” was a reality…it was happening! To my thinking…it was as if they were burying their heads in the sand, and pretending this just wasn’t happening! The mentality defied me!
Below is my original article with the articles now included. At the end is letters published regarding the “Bucking the Condomocracy” article, and a more recent article on the same subject. My bug chasing article can be found on this blog simply by searching for “barebacking”.
HIV Hyped
My, hasn’t the HIV community been blessed this month, with both a quarterly and a bi-monthly magazine taking up the HIV cause. I wish I could think that the sort of hype they give HIV/AIDS is harmless, but unfortunately, after reading through both articles – twice – just to make sure I hadn’t miss a subtle point, my conclusion is not so.
The article in HQ magazine (They Shoot Barebackers, Don’t They?), which has also received publicity via both the Sydney Star Observer, and the Sydney Morning Herald, is a reprint of an article from the American POZ magazine in February 1, 1999. When my partner and myself (also HIV+) read the article earlier this year, we were both quite horrified. It described in quite detailed account the so-called phenomena of ‘barebacking’, a current catch-cry for unsafe sex, especially between HIV positive and HIV negative men. This is supposedly by people who are ‘over’ practising safe sex and using condoms, and desire the thrill of ‘skin-to-skin’ sex. It reports on private parties in the USA for people who wish to indulge in this type of sex, and consider the risks of catching HIV minimal, compared to the joy of unprotected sex. Needless to say, the people who run the parties make sure everyone present signs a disclaimer. Wouldn’t want to get sued by people becoming infected, would we! The phenomena has reached as far as the Internet, where there are advertisements placed by HIV negative people to get HIV positive people to supposedly ‘father’ their own HIV infection. The mere implications of this sort of mentality would be enough to frighten anybody. There are also porn sites promoting galleries of photos with guys barebacking. Make it erotic, and you make it right, or so it would seem.
Of cause, the obvious question to ask is why is this happening? Have we stretched the limits of the practice and promotion of safe sex as far as it can go? Have people become so accepting of HIV that it is no longer considered a dangerous disease? Does the fact that we now have an arsenal of drugs to control HIV infection reducing people’s fear of infection? Do younger people consider the entire AIDS issue as a ‘generational’ thing? Is it just a millennium trend? Considering the current arguments going on around compliance and drug holidays, I don’t think it is feasible to even consider that HIV is either ended, or under control. Ask anyone infected and on drug regimes what they think of this! Ask them how much they enjoy taking the handfuls of pills everyday, and how much they enjoy the side effects of same. Ask them about how secure and comfortable they feel in the knowledge of a possible ten to twenty years with such regimes; always hoping the next generation of drugs is going to be easier on us. A vaccine is still a long way off.
Likewise, I also loved the article in ‘Blue” (“Bucking the Condomocracy”) which hit you in the face with the fabulous attention grabbing statement (in bold font) ‘POST-AIDS’. Now this article isn’t quite as bad as I originally thought. In the context in which it is written, it is in many respects correct. However, it does overlook a major point. If we are living with a ‘Post-AIDS’ mentality, then why are so many people in their mid twenties seroconverting? The article tends to cover the promise given by new treatments, but not the fact that playing down HIV is a dangerous road to take. It is full of trendy language, and as someone who has lived with HIV day in and day out for the last seventeen years, I haven’t heard of any of the expressions mooted by the author. Terms such as a ‘Protease Moment’, ‘vaccine optimism’ and ‘vaccine positive’ (in respect to forth coming language in the vaccine age) are all nice terms, and factually the article is right-there is more emphasis being placed on a preventative vaccine than a therapeutic, but that possibly is still a decade away. The article is, I grant you, full of positive images, which perhaps isn’t so bad in a world where doom and gloom are never far from the headlines. But it does seem to have made it look as though HIV is no longer happening. By being so nicey nicey about HIV, I feel it tends to play down the actual dangers inherent in contracting it. Again, ask anybody HIV positive if the would change sero status if possible, and you would get an almost one hundred percent resounding yes!
I felt, when originally reading the barebacking article earlier this year that it demanded a response, but being in an American magazine, and being a phenomena that I had not heard of occurring here (not, of cause, taking into account the many unsafe sex stories one hears from the saunas and backrooms), I decided to let it lie. The fact that HQ magazine has done a sideline on the Australian reaction to barebacking does not change the fact that, having the subject announced on the front cover is irresponsible journalism, to the extreme. The editor can defend it however she likes, but then she is not working in mainstream HIV/AIDS, and obviously knows very little about the subject, or the implications of the article. Trying to make barebacking a mainstream and fashionable pastime is not funny! An article published by Capital Q the same week as the SSO had its piece on HQ, showed the possible incidence of contracting HIV through unsafe sex. Odds of 120 to 1 (for unsafe anal) may sound good to many people, but considering the sex life of your average horny gay male, that makes the risk of infection from unsafe practices highly likely very early in their lives.
I grant that freedom of the press is a much-nurtured principle, but it can go too far, and the press often plays a major role in influencing people in a particular course of action that they may not otherwise take, and are often paramount in establishing new trends (Desirable, and undesirable). Journalists must stop looking at just headline stories to sell magazines, and consider the implications of what they are publishing.
LETTERS PUBLISHED IN “OUT” MAGAZINE SEPTEMBER 1999, VOL 8, NO. 3 IN RESPONSE TO “BUCKING THE CONDOMOCRACY”.
Barebacking is Dead. Long Live Barebacking!
Treasure Island Media
Leave it to science and rational thinking to ruin a popular sexual taboo.
The “bareback” label for sex without a condom has faded in the age of pre-exposure prophylaxis (PrEP) and U=U. People not living with HIV who are taking PrEP are protecting themselves from transmission, while people living with HIV who have an undetectable viral load are unable to transmit the virus to their sex partners at all. As the very definition of HIV risk is being rearranged, the problematic term “barebacking” is finally being relegated to the dust bins of history.
We all know the nature of taboo. The naughty, furtive longing for something forbidden. As the AIDS pandemic lurched from the murderous 80s into the 90s, sexual behavior among gay men pivoted, from horror at the very thought of sex without a condom to, well, something we just might like to do. Real bad. “Barebacking” instantly became part of the lexicon, spurred by maverick porn producers who capitalized on our carnal desire to have sex without a barrier.
Sex without a barrier. Unprotected sex. Barebacking. Also known as having sex. Ask a straight person.
Gay men have always barebacked, of course (along with every other human being and their parents), certainly before HIV ever showed up and yes, even immediately after. If we all had stopped fucking without barriers we would have halted the HIV epidemic in its tracks. Instead, we kept behaving like human beings, making mistakes or getting horny or saying yes when we should have said no or getting drunk or falling in love or being young and stupid.
And sometime, even in the darkest and deadliest years of the epidemic, to unload inside our partner was an enormous “fuck you” to AIDS. You might not understand the humanity of that choice, the triumph of it, or the search it represented for some kind of spiritual and physical release in the midst of relentless mortality. I guess you had to be there.
Not long after we emerged from the 1990s, shell shocked but ready to rumble openly again now that we were armed with effective medications, a renegade porn star bottom named Dawson collected orgasms in the double digits on video and his flick was so polarizing that it was banned in gay video stores. Today, his exploits seem positively quaint, and those same video stores and the countless internet sites that followed transformed themselves from featuring a barebacking category to dropping the category and lumping everything together. Sex without condoms in porn is now customary. Condoms are the outlier.
The actual term has lost its wicked luster. These days, you rarely hear your sex partner say, “oh yeah, fuck me bareback, man.” I mean, sure I will, dude. Yawn.
And gone, too, hopefully, is the judgment of those who labeled barebacking a deviant, destructive pathology. This may be the most painful aspect of our prevention legacy; the rush to demonize those who admitted to having sex without condoms before it became agreeable again, not to mention the furor over those of us who have spoken empathetically about sex without a barrier.
Activist and writer Tony Valenzuela became a community pariah when he wrote a piece in 1995 about being a young man living with HIV who had condomless sex with his boyfriend. He thumbed his nose at his detractors when he appeared naked on a horse for an infamous 1999 POZ Magazine cover (“They Shoot Barebackers, Don’t They?”) in which he discussed how the controversy angered and confused him. Valenzuela’s personal character was questioned and his professional life was derailed for years.
The late social anthropologist and author Eric Rofes (Reviving the Tribe) nearly caused a riot at a 1996 Atlanta town hall event for gay men when he discussed the spiritual and emotional value of sharing semen with a partner. And even as recently as 2013, my essay, “Your Mother Liked It Bareback,” produced one apoplectic comment, among many others, that remains the pinnacle of my blog infamy. “You,” it said, “are a vile merchant of death.”
Maybe, with our new biomedical tools of HIV prevention, those same people who once blindly damned sexual behaviors they didn’t understand — whether out of puritanical beliefs or their fear of their own desires – have reconciled their fantasies and their HIV risk. I hope they’re enjoying totally hot sex and the fluids are flying.
It is difficult to ignore the appalling homophobia, internalized and otherwise, that runs through this aspect of HIV prevention history. We held ourselves as gay men to a more grueling standard than the countless non-queers who get an STI (several of them life-threatening) or an unplanned pregnancy every year.
I have no illusions. Sexually transmitted infections continue, even if the very thought of gonorrhea just makes me feel nostalgic. The PrEP train hasn’t reached everyone who might benefit from it and there is misinformation about its efficacy and side effects. Meanwhile, nearly half of those living with HIV in the United States have not reached viral suppression. There is still reason to be cautious about the who and the when and the how of sex. Now, as ever, we are responsible for our own bodies and the risks we take.
Frankly, behavioral change has not served us well in the grand scheme of HIV prevention. There has always been some debate, tension even, between those who believed the answer to HIV infections is behavior modification, and those who welcome the advent of biomedical interventions such as PrEP and “treatment as prevention” (TasP) that don’t rely upon sexual behavioral choices to work.
Throughout the decades, we have all witnessed the dominant, primal pull that sexual desire has exhibited over caution, so I know which prevention strategy my money is on. But hey, to each his own strategy. For that matter, condoms are a golden oldie and a perfectly legitimate choice. You do you.
What has changed are the conversations and information gathering that happen between partners. PrEP, medications, who is undetectable or not, what sexual positioning in what combination will occur, all of these exist in a more informed landscape, at least among gay men in this country.
Barebacking, as an urban phrase and a taboo, is dead. Thank god and good riddance to this divisive bit of sexual branding. Sex, meanwhile, motors happily onward, unbothered by the judgments of man.
Eben Byers was an amateur golfer, an alumnus of Yale, and a notorious ladies man, but he is most famous for literally rotting from the inside out after spending three years drinking radium-infused water.
When Byers fell and hurt his arm in 1927, he was prescribed Radithor, a radium-infused elixir sold by a quack doctor named William Bailey. Radithor was supposed to alleviate aches, pains, and even invigorate one sexually. Yet what happened to Byers fell far afield of the positive effects Radithor was supposed to have. Instead, after three years of incessant use, Byers began rotting from the inside. His teeth fell out; his jaw had to be removed; holes formed in his brain and skull; and he eventually perished in 1932 from radium poisoning. Like the ill-fated Radium Girls before him, Byers demonstrated the clear and unequivocal bodily evidence that exposure to radium was lethal.
Byers’s tragic death is a story of medical deception and overdose, and it serves as a cautionary tale that there is, in fact, too much of a good thing – especially if that good thing is actually completely lethal.
“The Radium Water Worked Fine Until His Jaw Came Off”
This was the title of a Wall Street Journal article that came out some time after Byers’s passing, succinctly summing up what happened to him. In 1927, Byers was on a train returning from a Harvard-Yale football game when he fell from his bunk and hurt his arm. The pain didn’t go away, so Byers’s doctor prescribed him Radithor.
Radithor was simply radium dissolved in water, marketed as a healing tonic. At a time when radium-infused products were very popular, it was unsurprising that Byers was more than happy to take Radithor. In fact, Byers was so keen on the product and its supposed benefits that he ended up drinking three bottles every day for two years, until the poison caught up with him and began dissolving him from the inside out.
William Bailey, The Man Who Prescribed Byers Radithor, Was A Known Fraud
William J.A. Bailey wasn’t a doctor, even though he claimed to be. He was a Harvard dropout who got rich quick after developing Radithor, a toxic solution of radium dissolved in water. He was a fraud who was repeatedly in trouble with the law and profited off numerous short-lived business start-ups.
The FDA shut down Bailey’s business, but Bailey had already done his damage. The amount of people who perished from Radithor is unknown, but he sold approximately 400,000 bottles of the tonic – 1,400 of which Byers himself purchased.
Byers Probably Took Radithor To Help His Performance In The Bedroom
The quick story is that Byers fell on a train, hurt his arm, took Radithor, and thought it made him better so he kept taking it. There is, though, perhaps another reason Byers was so enthusiastic about Radithor, to the point where he reportedly even gave cases of the stuff to his girlfriends and his race horses.
Byers had a reputation as a ladies’ man. At Yale, his nickname was “Foxy Grandpa.” His fall on the train reportedly injured not only his arm, but also his game. Byers complained of a sort of “run-down feeling” that affected his athletic and sexual performance. That’s when Byers discovered a product on the market that claimed to solve all of these issues. The sexually reparative nature of Radithor was only rumored, but it is unsurprising that a man entering his 50s with a reputation for being popular with women would seek out anything to help him maintain his “Foxy Grandpa” status.
Byers’s Horrific Death Ended The American Public’s Romance With Radium-Infused Products
The problem with touting radioactivity as curative was that it simply wasn’t true. Luckily, most of these quack elixirs were phony, and contained no radium at all (of course, this was not the case with Radithor). Still, there were myriad products on the market meant to be extremely good for you – there were radium-infused beauty creams, toothpastes, soaps, bars of chocolates – you name it.
The American public had an obsession with radium in the 1920s and ’30s that only faded after Byers’s passing brought the real dangers of radium to light.
Byers’s Story Probably Got So Much Attention Because He Was A Handsome, Upper-Class Man
Eben Byers was the son of a well-known entrepreneur, and he was the chairman of his father’s steel company. He attended Yale, golfed, raced horses, and was popular with women. He was the perfect candidate for a tragic, newsworthy story – made even more fascinating and terrifying because he perished after drinking what was touted as a health tonic, completely available to the public. Everything about Byers’s story differs from the devastating story of the Radium Girls.
The tragedy of the Radium Girls – female factory employees who became painfully sick and perished of radium poisoning – was well covered by the media, but was less compelling to the government than the story of Byers, a socialite in the public eye. It wasn’t until Byers told the Federal Trade Commission about Radithor, while on his deathbed, that radium was removed from the federally approved list of medicines.
The Idea To Drink Radioactive Water As An Elixir Came From The Restorative Powers Of Hot Springs
In the 1920s, people knew about – and believed in – the healing powers of hot springs. When it was discovered that the water in hot springs was mildly radioactive, due to the radon gas dissolved in the water, it was concluded that it was the radioactivity that was so curative. In The American Journal of Clinical Medicine, Dr. C.G. Davis claimed, “Radioactivity prevents insanity, rouses noble emotions, retards old age, and creates a splendid youthful joyous life.” It was no wonder products infused with radium, such as candy, hair tonics, and even blankets, were so popular.
However, radon gas is entirely different from radium, the element found in Radithor. Radon gas has a half-life of about three days – radium has one of 1,600 years. Seeing as Byers took three times the already toxic dose of Radithor, he was irrevocably doomed.
Byers Deteriorated Rapidly and Painfully, But He Kept Drinking Radithor
For the first two years Byers took Radithor, he was so pleased with the supposed results that he took three times the suggested daily dose. But, after a while, he began feeling sick. He lost weight, had headaches, and had a blinding pain in his jaw. He had been diagnosed with inflamed sinuses, but once his teeth began to fall out and his jaw began to crumble, Byers knew something was terribly wrong. Byers’s X-ray was sent to a radiologist, who confirmed that Byers’s fate was inevitable – he had the same lesions on his jaw as the Radium Girls. Sadly, Byers was so indoctrinated to rely on Radithor that he kept drinking it, hoping it would help him feel better when he began feeling sick.
An attorney dispatched to Byers’s house shortly before his passing remembered the state Byers was in due to his radiation poisoning:
We went to Southampton where Byers had a magnificent home. There we discovered him in a condition which beggars description. Young in years and mentally alert, he could hardly speak. His head was swathed in bandages. He had undergone two successful jaw operations and his whole upper jaw, excepting two front teeth, and most of his lower jaw had been removed. All the remaining bone tissue of his body was slowly disintegrating, and holes were actually forming in his skull.
Byers Had Enough Radium In His Body To “Kill Three Men”
After Byers’s death, Popular Science Monthly wrote that Byers had the “largest amount of radium ever found in a human being – more than thirty micrograms, enough to kill three men.”
With symptoms such as blinding headaches, breaking bones, and a disintegrating jaw, Byers must have suffered immensely before he succumbed to radiation poisoning in 1932, five years after his first dose of Radithor.
The Federal Trade Commission Accidentally Contributed To The Rise Of Radioactive Products
Back when radium was immensely popular in consumer products, the FDA had very little power to regulate it. Not falling under food or drugs, it was out of their jurisdiction.
There was one department, however, that had control over radium: the Federal Trade Commission. Their job was to stand against false advertising claims; this meant that the FTC worked very hard to make sure that all the products on the market actually contained radium. Their strict regulation ensured that all the products people were buying were genuinely radioactive.
As Byers fell ill, and it became clear Radithor was the culprit, the FTC opened an investigation. They sought to challenge Bailey’s claim that Radithor and other products like it were “harmless.” They wanted Byers to testify, but he was too sick. They dispatched an attorney to his home to take a statement, which is when the attorney found him literally rotting from the inside out. It didn’t take long after that for the FTC to shut down Bailey’s business.
The results of the FTC’s investigation led to the FDA getting more power over investigating suspicious health claims. Eventually, the FDA gained control over the entire pharmaceutical industry.
Bailey Succumbed To His Own Lies, But It Was Only Discovered After His Death
Until the end, Bailey denied Radithor had anything to do with Byers’s demise. He claimed he had drunk more Radithor than Byers himself, and he was living proof that his “healing tonic” was perfectly safe.
Yet when his body was exhumed 20 years after his death from bladder cancer, medical researchers discovered his remains were riddled with radiation. His corpse was described as “still hot” after being unearthed.
Marie Curie and her husband, Pierre, discovered radium, a radioactive element, back in 1898. However, people didn’t realize how dangerous the element was, and they began to use radium in household items. This led to radium in makeup, as well as in medical devices that claimed to cure everything from impotence to arthritis. However, what these quack devices actually led to was a plethora of surprisingly poisonous things, such as toothpaste, hair tonic, and suppositories.
When people began dying of mysterious diseases, such as the ones suffered by the Radium Girls, who painted luminous watch dials with Undark, a radium-based paint that they wound up ingesting via their paintbrushes, doctors finally realized that radium was dangerous.
The history of radium poisoning is full of odd devices designed to improve one’s health and outer appearance. These everyday poisons were sold through magazine and newspaper ads – and in regular pharmacies. Thankfully, by the beginning of World War II, they had been phased out and are now an odd anecdote from American history.
Radium-Lined Cups Were Used To Make Radioactive Beverages
These days, people drink bottled or filtered water. Back in the early 20th century, those who could afford it drank radioactive water. One popular way of making this water, which supposedly could cure many different ailments, involved the use of a metal cup or container that was lined with radium. Any water poured into the vessel was exposed to the radioactive material and picked up its properties. The Revigator was one such device; its makers claimed that it contained radon. Of course, this only “worked” if the device actually contained radium – many of the “radioactive” medical marvels on the market were scams.
People Submerged Themselves In Radium-Laced Water At Spas
Going to spas and spending some time submerged in radioactive water was supposed to be an invigorating experience. In actuality, the natural radiation in these mineral hot springs might have made the spa goers feel relaxed – that is, until a few decades later when they realized that the “hot” water did more harm than good. During the time period, however, even reputable medical journals touted the healing abilities of radium and similar materials, and some claimed radium hot springs were a literal fountain of youth that could help slow the aging process. Some radium-filled hot springs are still in business today, but they limit people’s exposure to any radioactive elements in the water.
Laying In Radioactive Sand Was A Treatment For Arthritis
One of the main byproducts of radium manufacturing is a fine-grained sand that is, of course, highly radioactive. Back in the early 1900s, before people realized how harmful exposure to it was, they claimed that exposure to the sand could successfully treat arthritis pain. Many spas opened up rooms where people could sit and rest their feet on the sand in the hopes of being cured. The ironic thing is that, even though people knew of the dangers that radioactivity could pose, these “Uranium Sitting Houses” were in business up through the 1950s.
Men Placed Wax Coated Radium Rods In Their Urethras As A Cure For Impotence
Men have always struggled with impotence. Now, there are medications like Viagra; back in the early 1900s, there were “bougies.” These were radium-laced wax rods that men inserted directly into their urethras to treat impotence. This treatment is now cringe inducing not only because of the way it took place, but also because placing radioactive material close to reproductive organs is a very bad idea.
Radium Toothpaste Claimed To Make Teeth White And Shiny
Radium wasn’t just used in medical devices – it made its way into everyday beauty and household products as well. One of these hygienic products was toothpaste. According to ads, a small amount of radium in the toothpaste promised to make users’ teeth very white and super shiny. Whether or not it worked is up for debate, but what is known is that radioactive exposure can actually make one’s teeth fall out and result in a jaw rotting from the inside out.
Radithor Supposedly Cured Impotence And Other Health-Related Woes
Radithor was a radium- and thorium-laced water that was sold in small vials. A few drops of it a day could cure impotence and “restore vigor” – or, so it purported to be the case. The product was made by Bailey Radium Laboratories of East Orange, New Jersey, who actually encouraged users to disprove its claims of containing the radioactive substances. The product was removed from the market after one heavy user who reportedly went through around three vials a day of the stuff, playboy Eben Byers, died a horrific death when his jaw disintegrated.
Speaking of restoring “vigor,” how about a radium suppository? These small, radioactive pellets were sold in boxes and claimed to help men with their impotence issues. Made by several different companies, including the Vital-O-Gland Company and the General Remedies Company, there is no proof that the suppositories actually contained any radioactive material, or that they worked as they were supposed to. Thank goodness.
Glasses With Radioactive Lenses Corrected Vision Problems
Before there was laser eye surgery, there were Dengen’s Radio-Active Eye Applicators. This device looked like a pair of simple spectacles, only instead of lenses, it had opaque pods that contained radium and other radioactive materials. Not only could they cure your eye ailments, claiming to repair things like nearsightedness and farsightedness, but they also took care of headaches and eye strain. What’s even more disturbing is the fact the eye applicators came in three different strengths.
Tho-radia was a line of makeup and skin creams that contained radium. It was heavily marketed to women in the United States and France, who purchased the items in the hopes that the product’s claims – to rejuvenate and brighten skin – were true. To add a little extra cachet to the brand, its creator, Dr. Alfred Curie (no relation to Marie and Pierre Curie) put his name on the ads.
Radium bath salts, which worked like modern-day bath salts – as in you dissolve them in your bath water before soaking in them – were sold as a cure for insomnia, various nervous disorders, and even rheumatism. What made them even worse (from a modern perspective, of course) was the fact that dissolving the radioactive bath salts would send small particles of them into the air, where they were also breathed into the lungs. These products were made by several different manufacturers, including the Denver Radium Service on what is now a Superfund site.
Endocrine Glands Were Regulated With The Radiendocrinator
The endocrine system regulates the body’s hormone production. The glands in the endocrine system include those in the neck – the thyroid – as well as the pituitary gland in the brain. However, the horrifying detail here involves the glands that men would treat with the Radiendocrinator – their testes. Treatment via the Radiendocrinator involved holding the device in place sometimes for hours at a time, with the handy (and included) strap that resembled an athletic supporter. Ironically, the creator of the device, William J.A. Bailey, died of radiation-induced bladder cancer in 1949.
Gout And Neuralgia Were Taken Care Of With Radium Tablets
Radium tablets are still a legitimate medical treatment for people suffering from various types of cancer. However, back in the late 19th century, these tablets were sold on pharmacy shelves and supposedly cured gout, neuralgia (stabbing nerve pain), and numerous other ailments. These radioactive tablets, sold under brand names like Arium and Radione, were taken daily by people who simply wanted to feel better or have “the strength of iron.”
Radioactive Heating Pads Cured A Number Of Ailments
A radioactive heating pad that was lined with radium claimed to cure everything from rheumatism to standard aches and pains. The instructions for this particular device include warming it up, keeping it dry, and then applying it to the area of the body that hurts. Users could supposedly leave it on for up to 12 hours a day, and they were even encouraged to roll it up around a painful body part, such as an ankle, and tie it into place.
These days, uranium blankets are a part of nuclear reactors, and they aren’t even a little bit related to the therapeutic ones touted as cures for arthritis pain in the early 20th century. Those particular blankets looked like standard, quilted ones, only, within the fabric squares, were bits of uranium. These blankets were sold as cures up through the 1950s, even after the dangers of uranium exposure were well known.
A product called Caradium was created in the early 1900s. It was a tonic that was applied to hair to prevent gray hairs from growing, thanks to the power of its active ingredient – radium. It also promised to make any current gray hairs revert back to their old color. Caradium was the invention of Frederick Godfrey, a man whose credentials included “hair specialist.”
Vintage Shoe-Fitting X-Ray Machines Will Zap Your Feet
How do you tell if a shoe is a good fit? Take a short walk? Squeeze the front-end with your fingers to make sure there is space for your toes? What about a dangerous, 20-second blast of unshielded x-rays? If you were buying shoes in the 1930s, 1940s and 1950s, it’s likely that you regularly inserted a tootsie into one of these death-rays.
The wooden cabinets, possibly first built by a Clarence Karrer in Milwaukee in 1924, had the x-ray source in the base, and it would fire upwards through your foot and shoe. Due to a lack of any kind of shielding, it wouldn’t stop there: the radiation would shoot right up into your baby-maker, clearly a perilous occurrence.
The machine, called a “Shoe-Fitting Fluoroscope” put out 50 kv from its x-ray tube, which – according to Wikipedia’s figures for today’s machines, isn’t too bad:
In medical radiography voltage from 20 kV in mammography up to 150 kV for chest radiography are used for diagnostic. Energy can go up to 250 kV for radiotherapy applications.
The problem was repeat exposure. While it was recommended that children not be subjected to more than 12 doses a year, there was no such luck for shoe-store employees. According to the article Shoe-fitting with x-ray in National Safety News 62 by H. Bavley (1950), store clerks would put their hands into the beam to squeeze shoes during fitting. Worse still was the fate of a poor shoe model, “who received such a serious radiation burn that her leg had to be amputated.”
Thank God there’s nothing this dangerous around today. Like, you know, full-body backscatter x-ray machines in airports.
Get a reality check on some of the most bizarre rumours about how HIV is transmitted.
There’s only a few ways that you can get HIV but, at Avert, it seems that we’ve heard it all when it comes to the many myths and misconceptions about HIV.
A lot of these stories circulating on the HIV rumour mill are old, outdated and more importantly, misinformed. In fact, many of these myths just keep reinforcing HIV-related stigma and have had a long-lasting and damaging impact on many people’s perceptions about how the virus is spread.
Here we debunk some common urban legends to give you the truth about HIV transmission…
Myth 1: Girl goes to cinema and comes out with HIV
Rumour:During the 1990s, a common myth suggested that discarded needles left by strangers anywhere from gas pump handles to inside your cinema chair were infecting unassuming people with HIV. One such story involved a girl getting an unexpected needle stick injury while reaching down beneath her cinema seat to pick up some popcorn.
Reality:Although HIV transmission is a risk between people whoshare needles for drug use, there has actually never been a recorded case of HIV transmission from a discarded needle. However, if you are concerned that you have received a needle stick injury, you should seek medical advice to get checked up forhepatitis C andB instead.
Myth 2: There’s something wrong with this banana…
Rumour:Pictures of red-pigmented fruit (such as bananas or oranges) still circulate the web even today. They are usually accompanied by warnings not to eat them because they have supposedly been injected with HIV. Similar food-related HIV transmission rumours include tainted ketchup, pizza with toppings of bodily fluids and pineapple vendors accused of deliberately selling contaminated fruit.
Reality: You cannot get HIV from food of any kind, including fruit. Even if HIV contaminated blood did get onto the food you’re eating, the virus doesn’t live long enough outside of a human body for it to be transmittable.
Myth 3: I got a pedicure and HIV from some fish in a shopping centre
Rumour:Getting pedicures from Garra rufa fish – which nibble off dry skin – was once a popular beauty fad. However, many salons offering this service closed as a result of news outlets spreading the rumours that fish in these tanks were spreading blood-borne viruses such as HIV and hepatitis C between consumers.
Reality:HIV stands for Human Immunodeficiency Virus which means transmission of HIV only happens between humans – you can’t get HIV from animals, insects or fish. There are no cases of HIV infection due to the use of fish baths, or as a result of any other water-borne route including the use of swimming pools or spas.
Myth 4: The fizzy drink HIV hoax
Rumour:‘For the next few weeks do not drink any products from Pepsi, as a worker from the company has added his blood contaminated with HIV (AIDS)…’
This SMS message, which was falsely linked to the United Kingdom’s Metropolitan Police service in 2017, suggested that a line worker at Pepsi was secretly contaminating cans of fizzy drink with the virus.
Reality:This message has been circulating the web in different formats since 2004 and is incredibly damaging. Even if there was blood found within the drinks cans, HIV can’t live outside of the body long enough for it to be transmittable.
Myth 5: Teen diagnosed with HIV after getting a hair weave at salon
Rumour:In 2015, a rumour in the US reported that a girl in Georgia had contracted HIV at a hair salon because the needles used to fix the girl’s weave to her scalp were dirty. The girl was supposedly diagnosed a week after her makeover, despite never having had sex or used intravenous drugs.
Reality:This story was later reported to be a work of fiction by its author, but it is worth noting that transmission of HIV from stick injuries even in medical settings is extremely rare. The claim that someone can be diagnosed with HIV a week after exposure is also incorrect – as it can take from two weeks to 3 months for an infection to be detected by modern HIV tests.
There are still those out there who think AZT saved lives…it didn’t!I took it!I know!Will & Deni McIntyre—Getty Images
Today, if someone is diagnosed with HIV, he or she can choose among 41 drugs that can treat the disease. And there’s a good chance that with the right combination, given at the right time, the drugs can keep HIV levels so low that the person never gets sick.
That wasn’t always the case. It took seven years after HIV was first discovered before the first drug to fight it was approved by the U.S. Food and Drug Administration (FDA). In those first anxious years of the epidemic, millions were infected. Only a few thousand had died at that point, but public health officials were racing to keep that death rate from spiking — the inevitable result if people who tested positive weren’t treated with something.
As it turned out, their first weapon against HIV wasn’t a new compound scientists had to develop from scratch — it was one that was already on the shelf, albeit abandoned. AZT, or azidothymidine, was originally developed in the 1960s by a U.S. researcher as way to thwart cancer; the compound was supposed to insert itself into the DNA of a cancer cell and mess with its ability to replicate and produce more tumor cells. But it didn’t work when it was tested in mice and was put aside.
Two decades later, after AIDS emerged as new infectious disease, the pharmaceutical company Burroughs Wellcome, already known for its antiviral drugs, began a massive test of potential anti-HIV agents, hoping to find anything that might work against this new viral foe. Among the things tested was something called Compound S, a re-made version of the original AZT. When it was throw into a dish with animal cells infected with HIV, it seemed to block the virus’ activity.
The company sent samples to the FDA and the National Cancer Institute, where Dr. Samuel Broder, who headed the agency, realized the significance of the discovery. But simply having a compound that could work against HIV wasn’t enough. In order to make it available to the estimated millions who were infected, researchers had to be sure that it was safe and that it would indeed stop HIV in some way, even if it didn’t cure people of their infection. At the time, such tests, overseen by the FDA, took eight to 10 years.
Patients couldn’t wait that long. Under enormous public pressure, the FDA’s review of AZT was fast tracked — some say at the expense of patients.
Scientists quickly injected AZT into patients. The first goal was to see whether it was safe — and, though it did cause side effects (including severe intestinal problems, damage to the immune system, nausea, vomiting and headaches) it was deemed relatively safe. But they also had to test the compound’s effectiveness. In order to do so, a controversial trial was launched with nearly 300 people who had been diagnosed with AIDS. The plan was to randomly assign the participants to take capsules of the agent or a sugar pill for six months. Neither the doctor nor the patient would know whether they were on the drug or not.
After 16 weeks, Burroughs Wellcome announced that they were stopping the trial because there was strong evidence that the compound appeared to be working. One group had only one death. Even in that short period, the other group had 19. The company reasoned that it wouldn’t be ethical to continue the trial and deprive one group of a potentially life-saving treatment.
Those results — and AZT — were heralded as a “breakthrough” and “the light at the end of the tunnel” by the company, and pushed the FDA approve the first AIDS medication on March 19, 1987, in a record 20 months.
But the study remains controversial. Reports surfaced soon after that the results may have been skewed since doctors weren’t provided with a standard way of treating the other problems associated with AIDS — pneumonia, diarrhea and other symptoms — which makes determining whether the AZT alone was responsible for the dramatic results nearly impossible. For example, some patients received blood transfusions to help their immune systems; introducing new, healthy blood and immune cells could have helped these patients battle the virus better. There were also stories of patients from the 12 centers where the study was conducted pooling their pills, to better the chances that they would get at least some of the drug rather than just placebos.
And there were still plenty of questions left unanswered about the drug when it was approved. How long did the apparent benefits last? Could people who weren’t sick yet still benefit? Did they benefit more than those further along in their disease?
Such uncertainty would not be acceptable with a traditional approval, but the urgent need to have something in hand to fight the growing epidemic forced FDA’s hand. The people in the trial were already pressuring the company and the FDA to simply release the drug — if there were something that worked against HIV, they said, then it was not ethical to withhold it.
The drug’s approval remains controversial to this day, but in a world where treatment options are so far advanced it can be hard to imagine the sense of urgency and the social pressure permeating the medical community at the time. AIDS was an impending wave that was about to crash on the shores of an unsuspecting — and woefully unprepared — populace. Having at least one drug that worked, in however limited a way, was seen as progress.
But even after AZT’s approval, activists and public health officials raised concerns about the price of the drug. At about $8,000 a year (more than $17,000 in today’s dollars) — it was prohibitive to many uninsured patients and AIDS advocates accused Burroughs Wellcome of exploiting an already vulnerable patient population.
In the years since, it’s become clear that no single drug is the answer to fighting HIV. People taking AZT soon began showing rising virus levels — but the virus was no longer the same, having mutated to resist the drug. More drugs were needed, and AIDS advocates criticized the FDA for not moving quickly enough to approve additional medications. And side effects including heart problems, weight issues and more reminded people that anything designed to battle a virus like HIV was toxic.
Today, there are several classes of HIV drugs, each designed to block the virus at specific points in its life cycle. Used in combination, they have the best chance of keeping HIV at bay, lowering the virus’s ability to reproduce and infect, and ultimately, to cause death. These so-called antiretroviral drugs have made it possible for people diagnosed with HIV to live long and relatively healthy lives, as long they continue to take the medications.
And for most of these people, their therapy often still includes AZT.
AIDS HOPES DASHED BY TERRIBLE TRUTH ON AZT
It was the drug that held out hope to people carrying the world’s most feared virus. It had the power to move share prices by millions. What it could not do was help people facing AIDS.
This weekend the truth about AZT is in the open: a comprehensive trial, so big it equals all the other research put together, shows that the drug which dominates AIDS treatment has no effect in delaying the onset of the disease. After all the promise and the profits, AZT has nothing to offer people with HIV.
The findings came in the final report on the Anglo-French Concorde trial, published yesterday in The Lancet. Some 1,749 patients with HIV, but who showed no symptoms, were given either the drug or a placebo. There was no statistical difference in the progress of the two groups: after three years 18% had AIDS or were dead.
The results leave a terrible void for the 12m people worldwide said to be infected with the virus, and crush any remaining hopes that AZT might delay the onset of symptoms. They also raise questions as to how those hopes were fuelled in the first place.
Doubts about AZT were first revealed by The Sunday Times five years ago. A painstaking investigation showed that AZT had been rushed to market on the back of a flawed study that was supposed to demonstrate its effectiveness.
The American Food and Drug Administration (FDA), responsible for protecting the public from risk, had been aware of flaws in the trial, but gave AZT approval. Documents obtained under the American Freedom of Information Act showed that records compiled during the trial had been altered, giving the drug a more favourable record; “multiple deviations” from the terms of the study had occurred; and FDA investigators had argued for data from one centre to be dropped entirely from the results. A senior FDA official believed AZT should not be granted a licence, but was overruled.
The doubts did nothing to inhibit Wellcome, AZT’s maker, from promoting its drug. Patients with HIV, but without AIDS symptoms, were the new target. They are worth more money because there are more of them and because they have longer to live.
To show the drug’s usefulness to this lucrative group, Wellcome trumpeted a big American trial called Protocol 019. The trial was halted in August 1989, after less than two years, on the grounds that it had already shown such benefit to HIV-positive people it would be unethical not to give the drug to all who wanted it.
Such “benefit” was judged only by time free from disease. A new analysis of the trial data, however, reaches a similar conclusion to Concorde: that AZT is essentially useless.
The original results were announced with a fanfare by the National Institute of Allergy and Infectious Diseases, which sponsored it with Wellcome’s support. In London, The Independent newspaper gave its front page to the findings, under the headline “AIDS drug offers lease of life”.
The very different picture painted by last month’s analysis, in the New England Journal of Medicine, comes after investigators paid more attention to the drug’s side-effects. These can include anaemia, liver damage, fatigue, nausea, headaches and sometimes a collapse in white blood cells, making patients more prone to disease.
The researchers looked at the average time patients experienced neither a progression of disease nor an adverse effect. Those treated with low doses of AZT were found to suffer a reduction in quality of life “due to severe side-effects of therapy” that approximately equalled any benefit from slowing down the disease; people on higher doses suffered even greater side-effects, outweighing the supposed benefit.
Dr Peter Duesberg, the American virus expert who has claimed for years that AZT is not a rational therapy, says it is clear that the original claims were completely ill-founded. “The opposite interpretations of the same data lead me to conclude that those responsible are not acting as scientists; they are acting as politicians.
“When the time is ripe to say that AZT is detrimental, that it actually hurts, the interpretation will change again.”
For patients with AIDS-related symptoms, AZT will continue to be prescribed: the consensus remains that it gives a temporary benefit.
For those without symptoms, hope centres on combinations of drugs, or on other approaches such as gene therapy. However, Professor Ian Weller, of the Middlesex hospital in London, who was the principal British investigator in the Concorde trial, is alarmed by the drive to give AIDS patients an AZT drug cocktail as if it were already an established therapy.
“There’s a suspicion of more toxicity if you combine it with other treatment, and we are a long way from showing an important clinical benefit, or that it is safer than AZT on its own,” he said. “There are physicians who are jumping the gun.”
As late as Thursday, Wellcome was insisting that AZT “remains the best weapon we have to slow the progress of the disease”. Dr Trevor Jones, its research director, said: “The question is where in the course of the disease you begin.” *
AIDS and the AZT Scandal: SPIN’s 1989 Feature, ‘Sins of Omission’
The story of AZT, one of the most toxic, expensive, and controversial drugs in the history of medicine
At the end of 1989, two years after we had started the highly controversial AIDS column in SPIN, we published an article by Celia Farber called “Sins of Omission” about the truly bad and corrupt science surrounding promoting AZT as a treatment for the syndrome of diseases.
Celia was the editor and frequent writer of the column and unearthed hard evidence of the cold-bloodedness of the AIDS establishment pushing a drug that was worse than the disease, and killed faster than the natural progression of AIDS left untreated. AZT had been an abandoned cancer drug, discarded because of it’s fatal toxicity, resurrected in the cynical belief that AIDS patients were going to die anyway, so trying it out was sort of like playing with the house’s money. Because the drug didn’t require the usual massively expensive research and trial processes, having gone through that years earlier, it was insanely profitable for its maker, Burroughs Wellcome. It was a tragically perfect storm of windfall profits, something to pacify AIDS activists and the media, and a convenient boom to the patent holders for HIV testing.
Celia — who should get the Congressional Medal of Honor for her brave and relentless reporting, here and throughout the ten years we ran the column — exposed the worthlessness of the drug, the shady studies and deals to suppress the negative findings, and its awful and final consequences. This piece very literally changed the media’s view of AIDS and sharpened their discerning and skeptical eye. And soon after, AZT was once again shelved, hopefully this time forever.
Many times over the years since, people have come up to me and said that reading this article saved their lives, that they either stopped taking the drug and their health improved vastly, or they never took it because of what we reported. Nothing ever made me prouder.
— Bob Guccione Jr., founder of SPIN, October 3, 2015
[This story was originally published in the November 1989 issue of SPIN. In honor of SPIN’s 30th anniversary, we’ve republished this piece as part of our ongoing “30 Years, 30 Stories” series.]
On a cold January day in 1987, inside one of the brightly-lit meeting rooms of the monstrous FDA building, a panel of 11 top AIDS doctors pondered a very difficult decision. They had been asked by the FDA to consider giving lightning-quick approval to a highly toxic drug about which there was very little information. Clinically called Zidovudine, but nicknamed AZT after its components, the drug was said to have shown a dramatic effect on the survival of AIDS patients. The study that had brought the panel together had set the medical community abuzz. It was the first flicker of hope — people were dying much faster on the placebo than on the drug.
But there were tremendous concerns about the new drug. It had actually been developed a quarter of a century earlier as a cancer chemotherapy, but was shelved and forgotten because it was so toxic, very expensive to produce, and totally ineffective against cancer. Powerful, but unspecific, the drug was not selective in its cell destruction.
Drug companies around the world were sifting through hundreds of compounds in the race to find a cure, or at least a treatment, for AIDS. Burroughs Wellcome, a subsidiary of Wellcome, a British drug company, emerged as the winner. By chance, they sent the failed cancer drug, then known as Compound S, to the National Cancer Institute along with many others to see if it could slay the AIDS dragon, HIV. In the test tube at least, it did. At the meeting, there was a lot of uncertainty and discomfort with AZT. The doctors who had been consulted knew that the study was flawed and that the long-range effects were completely unknown. But the public was almost literally baying at the door. Understandably, there was immense pressure on the FDA to approve AZT, considering the climate of fear and anger all around.*
Everybody was worried about this one. To approve it, said Ellen Cooper, an FDA director, would represent a “significant and potentially dangerous departure from our normal toxicology requirements.” Just before approving the drug, one doctor on the panel, Calvin Kunin, summed up their dilemma. “On the one hand,” he said, “to deny a drug which decreases mortality in a population such as this would be inappropriate. On the other hand, to use this drug widely, for areas where efficacy has not been demonstrated, with a potentially toxic agent, might be disastrous.”
“We do not know what will happen a year from now,” said panel chairman Dr. Itzhak Brook. “The data is just too premature, and the statistics are not really well done. The drug could actually be detrimental.” A little later, he said he was also “struck by the fact that AZT does not stop deaths. Even those who were switched to AZT still kept dying.”
“I agree with you,” answered another panel member, “there are so many unknowns. Once a drug is approved, there is no telling how it could be abused. There’s no going back.” Burroughs Wellcome reassured the panel that they would provide detailed two-year follow-up data, and that they would not let the drug get out of its intended parameters: as a stopgap measure for very sick patients.
Dr. Brook was not won over by the promise. “If we approve it today, there will not be much data. There will be a promise of data,” he predicted, “but then the production of data will be hampered.” Brook’s vote was the only one cast against approval.
“There was not enough data, not enough follow-up,” Brook recalls. “Many of the questions we asked the company were answered by, ‘We have not analyzed the data yet,’ or, ‘We do not know.’ I felt that there was some promising data, but was very worried about the price being paid for it. The side effects were so very severe. It was chemotherapy. Patients were going to need blood transfusions, that’s very serious.”
“The committee was tending to agree with me,” says Brook, “that we should wait a little bit, be more cautious. But once the FDA realized we were intending to reject it, they applied political pressure. At about 4 p.m., the head of the FDA’s Center for Drugs and Biologics asked permission to speak, which is extremely unusual. Usually they leave us alone. But he said to us, ‘Look, if you approve the drug, we can assure you that we will work together with Burroughs Wellcome and make sure the drug is given to the right people.’ It was like saying ‘please do it.’”
Brad Stone, FDA press officer, was at that meeting. He says he doesn’t recall that particular speech, but that there is nothing “unusual” about FDA officials making such speeches at advisory meetings. “There was no political pressure,” he says. “The people in that meeting approved the drug because the data the company had produced proved it was prolonging life. Sure it was toxic, but they concluded that the benefits clearly outweighed the risks.” The meeting ended. AZT, which several members of the panel still felt uncomfortable with and feared could be a time bomb, was approved.
Flash forward: August 17, 1989. Newspapers across America banner-headlined that AZT had been “proven to be effective in HIV antibody-positive, asymptomatic, and early ARC patients,” even though one of the panel’s main concerns was that the drug should only be used in a last-case scenario for critically-ill AIDS patients, due to the drug’s extreme toxicity. Dr. Anthony Fauci, head of the National Institutes of Health (NIH), was now pushing to expand prescription.
The FDA’s traditional concern had been thrown to the wind. Already the drug had spread to 60 countries and an estimated 20,000 people. Not only had no new evidence allayed the initial concerns of the panel, but the follow-up data, as Dr. Brook predicted, had fallen by the wayside. The beneficial effects of the drug had proven to be temporary. The toxicity, however, stayed the same.
The majority of those in the AIDS-afflicted and medical communities held the drug up as the first breakthrough on AIDS. For better or worse, AZT had been approved faster than any drug in FDA history, and activists considered it a victory. The price paid for the victory, however, was that almost all government drug trials, from then on, focused on AZT — while over 100 other promising drugs were left uninvestigated.
Burroughs Wellcome stock went through the roof when the announcement was made. At a price of $8.000 per patient per year (not including blood-work and transfusions), AZT is the most expensive drug ever marketed. Burroughs Wellcome’s gross profits for next year are estimated at $230 million. Stock market analysts predict that Burroughs Wellcome may be selling as much as $2 billion worth of AZT, under the brand name Retrovir, each year by the mid-1990s — matching Burroughs Wellcome’s total sales for all its products last year.
“Does AZT do anything? Yes, it does. But the evidence that it does something against HIV is really not there.”
AZT is the only antiretroviral drug that has received FDA approval for treatment of AIDS since the epidemic began ten years ago, and the decision to approve it was based on a single study that has long been declared invalid. The study was intended to be a “double-blind placebo-controlled study,” the only kind of study that can effectively prove whether or not a drug works. In such a study, neither patient nor doctor is supposed to know if the patient is getting the drug or a placebo. In the case of AZT, the study became unblinded on all sides, after just a few weeks.
Both sides contributed to the unblinding. It became obvious to doctors who was getting what because AZT causes such severe side effects that AIDS per se does not. Furthermore, a routine blood count known as a CMV, which clearly shows who is on the drug and who is not, wasn’t whited out in the reports. Both of these facts were accepted and confirmed by both the FDA and Burroughs Wellcome, who conducted the study.
Many of the patients who were in the trial admitted that they had analyzed their capsules to find out whether they were getting the drug. If they weren’t, some bought the drug on the underground market. Also, the pills were supposed to be indistinguishable by taste, but they were not. Although this was corrected early on, the damage was already done. There were also reports that patients were pooling pills out of solidarity to each other. The study was so severely flawed that its conclusions must be considered, by the most basic scientific standards, unproven.
The most serious problem with the original study, however, is that it was never completed. Seventeen weeks into the study, when more patients had died in the placebo group, the study was stopped, five months prematurely, for “ethical” reasons: It was considered unethical to keep giving people a placebo when the drug might keep them alive longer. Because the study was stopped short, and all subjects were put on AZT, no scientific study can ever be conducted to prove unequivocally whether AZT does prolong life.
Dr. Brook, who voted against approval, warned at the time that AZT, being the only drug available for doctors to prescribe to AIDS patients, would probably have a runaway effect. Approving it prematurely, he said, would be like “letting the genie out of the bottle.”
Brook pointed out that since the drug is a form of chemotherapy, it should only be prescribed by doctors who have experience with chemotherapeutic drugs. Because of the most severe toxic effect of AZT — cell depletion of the bone marrow —patients would need frequent blood transfusions. As it happened, AZT was rampantly prescribed as soon as it was released, way beyond its purported parameters. The worst-case scenario had come true: Doctors interviewed by the New York Times later in 1987 revealed that they were already giving AZT to healthy people who had tested positive for antibodies to HIV.
The FDA’s function is to weigh a drug’s efficacy against its potential hazards. The equation is simple and obvious: A drug must unquestionably repair more than it damages, otherwise the drug itself may cause more harm than the disease it is supposed to fight. Exactly what many doctors and scientists fear is happening with AZT.
“I personally do not prescribe AZT. I have continued to experience that people live longer who are not on it.”
AZT was singled out among hundreds of compounds when Dr. Sam Broder, the head of the National Cancer Institute (NCI), found that it “inhibited HIV viral replication in vitro.” AIDS is considered a condition of immune suppression caused by the HIV virus replicating and eating its way into T-4 cells, which are essential to the immune system. HIV is a retrovirus which contains an enzyme called reverse transcriptase that converts viral RNA to DNA. AZT was thought to work by interrupting this DNA synthesis, thus stopping further replication of the virus.
While it was always known that the drug was exceedingly toxic, the first study concluded that “the risk/benefit ratio was in favor of the patient.”
In the study that won FDA approval for AZT, the one fact that swayed the panel of judges was that the AZT group outlived the placebo group by what appeared to be a landslide. The ace card of the study, the one that canceled out the issue of the drug’s enormous toxicity, was that 19 persons had died in the placebo group and only one in the AZT group. The AZT recipients were also showing a lower incidence of opportunistic infections.
While this data staggered the panel that approved the drug, other scientists insisted that it meant nothing — because it was so shabbily gathered, and because of the unblinding. Shortly after the study was stopped, the death rate accelerated in the AZT group. “There was no great difference after a while,” says Dr. Brook, “between the treated and the untreated group.”
“That study was so sloppily done that it really didn’t mean much,” says Dr. Joseph Sonnabend, a leading New York City AIDS doctor. Dr. Harvey Bialy, scientific editor of the journal Biotechnology, is stunned by the low quality of science surrounding AIDS research. When asked if he had seen any evidence of the claims made for AZT, that it “prolongs life” in AIDS patients, Bialy said, “No, I have not seen a published study that is rigorously done, analyzed, and objectively reported.”
Bialy, who is also a molecular biologist, is horrified by the widespread use of AZT, not just because it is toxic, but because, he insists, the claims its widespread use are based upon are false. “I can’t see how this drug could be doing anything other than making people very sick,” he says.
The scientific facts about AZT and AIDS are indeed astonishing. Most ironically, the drug has been found to accelerate the very process it was said to prevent: the loss of T-4 cells.
“Undeniably, AZT kills T-4 cells [white blood cells vital to the immune system],” says Bialy. “No one can argue with that. AZT is a chain-terminating nucleotide, which means that it stops DNA replication. It seeks out any cell that is engaged in DNA replication and kills it. The place where most of this replication is taking place is in the bone marrow. That’s why the most common and severe side effect of the drug is bone marrow toxicity. That is why they [patients] need blood transfusions.”
AZT has been aggressively and repeatedly marketed as a drug that prolongs survival in AIDS patients because it stops the HIV virus from replicating and spreading to healthy cells. But, says Bialy: “There is no good evidence that HIV actively replicates in a person with AIDS, and if there isn’t much HIV replication to stop, it’s mostly killing healthy cells.”
University of California at Berkeley scientist Dr. Peter Duesberg drew the same conclusion in a paper published in Proceedings, the journal of the National Academy of Sciences. Duesberg, whose paper addressed his contention that HIV is not a sufficient cause for AIDS, wrote: “Even if HIV were to cause AIDS, it would hardly be a legitimate target for AZT therapy, because in 70 to 100 percent of antibody-positive persons, proviral DNA is not detectable… and its biosynthesis has never been observed.”
As a chemotherapeutic drug, explained Duesberg, AZT “kills dividing blood cells and other cells,” and is thus “directly immunosuppressive.”
“The cell is almost a million-fold bigger target than the virus, so the cell will be much, much more sensitive,” says Duesberg. “Only very few cells, about one in 10,000, are actively making the virus containing DNA, so you must kill incredibly large numbers of cells to inhibit the virus. This kind of treatment could only theoretically help if you have a massive infection, which is not the case with AIDS. Meanwhile, they’re giving this drug that ends up killing millions of lymphocytes [white blood cells]. It’s beyond me how that could possibly be beneficial.”
“It doesn’t really kill them,” Burroughs Wellcome scientist Sandra Lehrman argues. “You don’t necessarily have to destroy the cell, you can just change the function of it. Furthermore, while the early data said that only very few cells were infected, new data says that there may be more cells infected. We have more sensitive detection techniques now.”
“Changes their function? From what — functioning to not functioning? Another example of mediocre science,” says Bialy. “The ‘sensitive detection technique’ to which Dr. Lehrman refers, PCR, is a notoriously unreliable one upon which to base quantitative conclusions.”
When specific questions about the alleged mechanisms of AZT are asked, the answers are long, contradictory, and riddled with unknowns. Every scientific point raised about the drug is eventually answered with the blanket response, “The drug is not perfect, but it’s all we have right now.” About the depletion of T-4 cells and other white cells, Lehrman says, “We don’t know why T-4 cells go up at first, and then go down. That is one of the drug mechanisms that we are trying to understand.”
When promoters of AZT are pressed on key scientific points, whether at the NIH, FDA, Burroughs Wellcome, or an AIDS organization, they often become angry. The idea that the drug is “doing something,” even though this is invariably followed with irritable admissions that there are “mechanisms about the drug and disease we don’t understand,” is desperately clung to. It is as if, in the eye of the AIDS storm, the official, government-agency sanctioned position is immunized against critique. Skepticism and challenge, so essential to scientific progress and so prevalent in every other area of scientific endeavor, is not welcome in the AZT debate, where it is arguably needed more than anywhere else.
The results, finally and ironically, are what damns AZT.
The toxic effects of AZT, particularly bone marrow suppression and anemia, are so severe that up to 50 percent of all AIDS and ARC patients cannot tolerate it and have to be taken off it. In the approval letter that Burroughs Wellcome sent to the FDA, all of 50 additional side effects of AZT, aside from the most common ones, were listed. These included: loss of mental acuity, muscle spasms, rectal bleeding, and tremors.
Anemia, one of AZT’s common side effects, is the depletion of red blood cells, and, according to Duesberg, “Red blood cells are the one thing you cannot do without. Without red cells, you cannot pick up ???gen.”
Fred, a person with AIDS, was put on AZT and suffered such severe anemia from the drug he had to be taken off it. In an interview in the AIDS handbook Surviving and Thriving With AIDS, he described what anemia feels like to editor Michael Callen: “I live in a studio and my bathroom is a mere five-step walk from my bed. I would just lie there for two hours; I couldn’t get up to take those five steps. When I was taken to the hospital, I had to have someone come over to dress me. It’s that kind of severe fatigue. The quality of my life was pitiful… I’ve never felt so bad… I stopped the AZT and the mental confusion, the headaches, the pains in the neck, the nausea, all disappeared within a 24-hour period.”
“I feel very good at this point,” Fred went on. “I feel like the quality of my life was a disaster two weeks ago. And it really was causing a great amount of fear in me, to the point where I was taking sleeping pills to calm down. I was so worried. I would totally lose track of what I was saying in the middle of a sentence. I would lose my directions on the street.”
“Many AIDS patients are anemic even before they receive the drug,” says Burroughs Wellcome’s Dr. Lehrman, “because HIV itself can infect the bone marrow and cause anemia.”
This argument betrays a bizarre reasoning. If AIDS patients are already burdened with problems such as immune suppression, bone marrow toxicity, and anemia, is compounding these problems an improvement?
“Yes, AZT is a form of chemotherapy,” says the man who invented the compound a quarter-century ago, Jerome Horwitz. “It is cytotoxic, and as such, it causes bone marrow toxicity and anemia. There are problems with the drug. It’s not perfect. But I don’t think anybody would agree that AZT is of no use. People can holler from now until doomsday that it is toxic, but you have to go with the results.”
The results, finally and ironically, are what damns AZT. Several studies on the clinical effects of AZT — including the one that Burroughs Wellcome’s approval was based on — have drawn the same conclusion: that AZT is effective for a few months, but that its effect drops off sharply after that. Even the original AZT study showed that T-4 cells went up for a while and then plummeted. HIV levels went down, and then came back up. This fact was well-known when the advisory panel voted for approval. As panel member Dr. Stanley Lemon said in the meeting, “I am left with the nagging thought that after seeing several of these slides, that after 16 to 24 weeks — 12 to 16 weeks, I guess — the effect seems to be declining.”
A follow-up meeting, two weeks after the original Burroughs Wellcome study, was scheduled to discuss the long-range effects of AZT and the survival statistics. As one doctor present at that meeting in May 1988 recalls, “They hadn’t followed up the study. Anything that looked beneficial was gone within half a year. All they had were some survival statistics averaging 44 weeks. The p24 didn’t pan out and there no persistent improvement in T-4 cells.”
HIV levels in the blood are measured by an antigen called p24. Burroughs Wellcome made the claim that AZT lowered this level, that is, lowered the amount of HIV in the blood. At the first FDA meeting, Burroughs-Welcome emphasized how the drug had “lowered” the p24 levels; at the follow-up meeting they didn’t even mention it.
As that meeting was winding down, Dr. Michael Lange, head of the AIDS program at St. Luke’s-Roosevelt Hospital in New York spoke up about this. “The claim of AZT is made on the fact that it is supposed to have an antiviral effect,” he said to Burroughs Wellcome, “and on this we have seen no data at all… Since there is a report in the Lancet [a leading British medical journal] that after 20 weeks or so, in many patients p24 came back, do you have any data on that?”
They didn’t.
“What counts is the bottom line,” one of the scientists representing Burroughs Wellcome summed up, “the survival, the neurologic function, the absence of progression and the quality of life, all of which are better. Whether you call it better because of some antiviral effect, or some other antibacterial effect, they are still better.”
Dr. Lange suggested that the drug may be effective in the same way a simple anti-inflammatory, such as aspirin, is effective. An inexpensive, nontoxic drug called Indomecithin, he pointed out, might serve the same function, without the devastating side effects.
One leading AIDS researcher, who was part of the FDA approval process, says today: “Does AZT do anything? Yes, it does. But the evidence that it does something against HIV is really not there.”
“There have always been drugs that we use without knowing exactly how they work,” says Nobel Prize winner Walter Gilbert. “The really important thing to look at is the clinical effect. Is the drug helping or isn’t it?”
A physician with extensive experience with AIDS patients who asked to remain anonymous told SPIN, point blank: “I personally do not prescribe AZT. I have continued to experience that people live longer who are not on it.”
“I’m living proof that AZT works,” says one person with ARC on AZT. “I’ve been on it for two years now, and I’m certainly healthier than I was two years ago. It’s not a cure-all, it’s not a perfect drug, but it’s effective. It’s slowing down the progression of the disease.”
“Sometimes I fee like I’m swallowing Drano,” says another. “I mean, sometimes I have problems swallowing. I just don’t like the idea of taking something that foreign to my body. But every six hours, I’ve got to swallow it. Until something better comes along, this is what is available to me.”
“I am absolutely convinced that people enjoy a better quality of life and survive longer who do not take AZT,” says Gene Fedorko, President of Health Education AIDS Liaison (HEAL). “I think it’s horrible the way people are bullied by their doctors to take this drug. We get people coming to us shaking and crying because their doctors said they’ll die if they don’t take AZT. That is an absolute lie.” Fedorko has drawn his conclusion from years of listening to the stories of people struggling to survive AIDS at HEAL’s weekly support group.
“I wouldn’t take AZT if you paid me,” says Michael Callen, cofounder of New York City’s PWA coalition, Community Research Initiative, and editor of several AIDS journals. Callen has survived AIDS for over seven years without the help of AZT. “I’ve gotten the s–t kicked out of me for saying this, but I think using AZT is like aiming a thermonuclear warhead at a mosquito. The overwhelming majority of long-term survivors I’ve known have chosen not to take AZT.”
“I’m convinced that if you gave AZT to a perfectly healthy athlete he would be dead in five years.”
The last surviving patient from the original AZT trial, according Burroughs Wellcome, died recently. When he died, he had been on AZT for three and one-half years. He was the longest surviving AZT recipient. The longest surviving AIDS patient overall, not on AZT, has lived for eight and one-half years.
An informal study of long-term survivors of AIDS followed 24 long-term survivors, all of whom had survived AIDS for more than six years. Only one of them had recently begun taking AZT.
In the early days, AZT was said to extend lives. In actual fact, there is simply no solid evidence that AZT prolongs life.
“I think AZT does prolong life in most people,” says Dr. Bruce Montgomery of the State University of New York at Stony Brook, who is completing a study on AZT. “There are not very many long-term survivors, and we really don’t know why they survive. It could be luck. But most people are not so lucky.”
“AZT does seem to help many patients,” says Dr. Bernard Bahari, a New York City AIDS physician and researcher, “but it’s very hard to determine whether it actually prolongs life.”
“Many of the patients I see choose not to take AZT,” says Dr. Don Abrams of San Francisco General Hospital. “I’ve been impressed that survival and lifespan are increasing for all people with AIDS. I think it has a lot to do with aerosolized Pentamadine [a drug that treats pneumocystis carinii pneumonia]. There’s also the so-called plague effect, the fact that people get stronger and stronger when a disease hits a population. The patients I see today are not as fragile as the early patients were.”
“Whether you live or die with AIDS is a function of how well your doctor treats you, not of AZT,” says Dr. Joseph Sonnabend, one of New York City’s first and most reputable AIDS doctors, whose patients include many long-term survivors, although he has never prescribed AZT. Sonnabend was one of the first to make the simple observation that AIDS patients should be treated for their diseases, not just for their HIV infection.
Several studies have concluded that AZT has no effect on the two most common opportunistic AIDS infections, Pneumocystic Carinii Pneumonia (PCP) and Kaposi’s Sarcoma (KS). The overwhelming majority of AIDS patients die of PCP, for which there has been an effective treatment for decades. This year, the FDA finally approved aerosolized Pentamadine for AIDS. A recent Memorial Sloan Kettering study concluded the following: By 15 months, 80 percent of people on AZT not receiving Pentamadine had a recurrent episode of pneumocystis. Only 5 percent of those people who did get Pentamadine had a recurring episode. “All those deaths in the AZT study were treatable,” Sonnabend says. “They weren’t deaths from AIDS, they were deaths from treatable conditions. They didn’t even do any autopsies for that study. What kind of faith can one have in these people?”
“If there’s one resistance to AZT in the general public at all, it’s within the gay community of New York,” says the doctor close to the FDA approval, who asked to remain anonymous. “The rest of this country has been brainwashed into thinking this drug really does that much. The data has all been manipulated by people who have a lot vested in AZT.”
“If AIDS were not the popular disease that it is — the money-making and career-making machine — these people could not get away with this kind of shoddy science,” says Bialy. “In all my years in science I have never seen anything this atrocious.” When asked if he thought it was at all possible that people have been killed as a result of AZT poisoning rather than AIDS he answered: “It’s more than possible.”
August 17, 1989: The government has announced that 1.4 million healthy, HIV antibody-positive Americans could “benefit” from taking AZT, even though they show no symptoms of disease. New studies have “proven” that AZT is effective in stopping the progression of AIDS in asymptomatic and early ARC cases. Dr. Fauci, the head of NIH, proudly announced that a trial has been going on for “two years” had “clearly shown” that early intervention will keep AIDS at bay. Anyone who has antibodies to HIV and less than 500 T-4 cells should start taking AZT at once, he said. That is approximately 650,000 people. 1.4 million Americans are assumed HIV antibody-positive, and eventually all of them may need to take AZT so they don’t get sick, Fauci contended.
The leading newspapers didn’t seem to think it unusual that there was no existing copy of the study, but rather a breezy two-page press release from the NIH. When SPIN called the NIH asking for a copy of the study, we were told that it was “still being written.”
We asked a few questions about the numbers. According to the press release, 3,200 early ARC and asymptomatic patients were divided into two groups, one AZT and one placebo, and followed for two years. The two groups were distinguished by T-4 cell counts; one group had less than 500, the other more than 500. These two were then divided into three groups each: high-dose AZT, low-dose AZT, and placebo. In the group with more than 500 T-4 cells, AZT had no effect. In the other group, it was concluded that low-dose AZT was the most effective, followed by high-dose. All in all, 36 out of 900 developed AIDS in the two AZT groups combined, and 38 out of 450 in the placebo group. “HIV-positive are twice as likely to get AIDS if they don’t take AZT,” the press declared.
However, the figures are vastly misleading. When we asked how many patients were actually enrolled for a full two years, the NIH said they did not know, but that the average time of participation was one year, not two.
“It’s terribly dishonest the way they portrayed those numbers,” says Dr. Sonnabend. “If there were 60 people in the trial those numbers would mean something, but if you calculate what the percentage is out of 3,200, the difference becomes minute between the two groups. It’s nothing. It’s hit or miss, and they make it look like it’s terribly significant.”
The study boasted that AZT is much more effective and less toxic at one-third the dosage than has been used for three years now. That’s the good news. The bad news is that thousands have already been walloped with 1,500 milligrams of AZT and possibly even died of toxic poisoning — and now we’re hearing that one third of the dose would have done?
With all that remains so uncertain about the effects of AZT, it seems criminal to advocate expanding its usage to healthy people, particularly since only a minuscule percentage of the HIV-infected population have actually developed ARC or AIDS.
Burroughs Wellcome has already launched testing of AZT in asymptomatic hospital workers, pregnant women, and in children, who are getting liquid AZT. The liquid is left over from an aborted trial, and given to the children because they can mix it with water — children don’t like to swallow pills. It has also been proposed that AZT be given to people who do not yet even test positive for HIV antibodies, but are “at risk.”
“I’m convinced that if you gave AZT to a perfectly healthy athlete,” says Fedorko, “he would be dead in five years.”
“This is such shoddy science it’s hard to believe nobody is protesting.”
In December 1988, the Lancet published a study that Burroughs Wellcome and the NIH do not include in their press kits. It was more expansive than the original AZT study and followed patients longer. It was not conducted in the United States, but in France, at the Claude Bernard Hospital in Paris, and concluded the same things about AZT that Burroughs Wellcome’s study did, except Burroughs Wellcome called their results “overwhelmingly positive,” and the French doctors called theirs “disappointing.” The French study found, once again, that AZT was too toxic for most to tolerate, had no lasting effect on HIV blood levels, and left the patients with fewer T-4 cells than they started with. Although they noticed a clinical improvement at first, they concluded that “by six months, these values had returned to their pretreatment levels, and several opportunistic infections, malignancies, and deaths occurred.”
“Thus the benefits of AZT are limited to a few months for ARC and AIDS patients,” the French team concluded. After a few months, the study found, AZT was completely ineffective.
The news that AZT will soon be prescribed to asymptomatic people has left many leading AIDS doctors dumbfounded and furious. Every doctor and scientist I asked felt that it was highly unprofessional and reckless to announce a study with no data to look at, making recommendations with such drastic public health implications. “This simply does not happen,” says Bialy. “The government is reporting scientific facts before they’ve been reviewed? It’s unheard of.”
“It’s beyond belief,” says Dr. Sonnabend in a voice tinged with desperation. “I don’t know what to do. I have to go in and face an office full of people asking for AZT. I’m terrified. I don’t know what to do as a responsible physician. The first study was ridiculous. Margaret Fischl, who has done both of these studies, obviously doesn’t know the first thing about clinical trials. I don’t trust her. Or the others. They’re simply not good enough. We’re being held hostage by second-rate scientists. We let them get away with the first disaster; now they’re doing it again.”
“It’s a momentous decision to say to people, ‘If you’re HIV-positive and your T-4 cells are below 500, start taking AZT,’” says the AIDS doctor who wished to remain anonymous. “I know dozens of people that I’ve seen personally every few months for several years now who have been in that state for more than five years, and have not progressed to any disease.”
“I’m ashamed of my colleagues,” Sonnabend laments. “I’m embarrassed. This is such shoddy science it’s hard to believe nobody is protesting. Damned cowards. The name of the game is to protect your grant, don’t open your mouth. It’s all about money… it’s grounds for just following the party line and not being critical, when there are obviously financial and political forces driving this.”
When Duesberg heard the latest announcement, he was partially stunned over the reaction of Gay Men’s Health Crisis President Richard Dunne, who said that GMHC now urged “everybody to get tested,” and of course those who test positive to go on to AZT. “These people are running into the gas chambers,” says Duesberg. “Himmler would have been so happy if only the Jews were this cooperative.”
* = This sentence was changed to correct an error in the original version of this article, which wrongly stated that the FDA had approved Thalidomide.
The rise and fall of AZT: It was the drug that had to work. It brought hope to people with HIV and Aids, and millions for the company that developed it. It had to work. There was nothing else. But for many who used AZT – it didn’t
RUMOURS about the drug had been circulating since early 1985 when word came from America that a company in Carolina had found a compound that was effective against HIV – at least in a Petri dish. Two years later, by the time AZT had been licensed for use, demand for it had grown to gigantic proportions.
By then, Aids patients had grown so desperate that they would sample any of the bootlegged underground therapies, some of which were probably life-threatening. With the arrival of AZT, doctors who had been powerless for so long against a syndrome about which they knew so little, at last had something they could give their patients that had passed stringent official tests.
In March 1987, when AZT was available on prescription for the first time, almost everyone with Aids wanted to take it, as did many who had tested positive for HIV. One of these was Michael Cottrell, a gay Englishman. He had tested positive for HIV in 1985 at the age of 22. He took AZT for several months in the late Eighties and suffered severe side-effects from the drug: chronic headaches and nausea, debilitating muscle fatigue. Cottrell felt much worse on AZT than he did off it. But he persevered because it seemed AZT was the only anti-Aids drug there was.
So Cottrell took it early in his infection: after all, if AZT was judged to be effective in treating Aids, then perhaps, it was thought, it would also benefit those who took it before they became ill. AZT spelt hope: psychologically it served to dispel despair. It was never claimed to be a cure, but it did claim to keep you alive longer, and in that extra time it bought, who knew what would happen? Maybe a cure would be found. Maybe a vaccine. Maybe other drugs would be developed to fight the disease, too.
Cottrell still has boxes of AZT capsules at home. He gave up on it after several months, because he couldn’t stand how ill he was feeling on the drug; he felt as though his immune system was being damaged rather than strengthened; he believed he had never encountered a drug as toxic as AZT.
Cottrell knew the drug didn’t work for him, but he believed he might have been one of the unlucky ones, like people who react badly to penicillin. Then a month ago he woke up to the news that the drug didn’t work on HIV at all, and that all his suffering had been avoidable.
Concorde, an Anglo-French programme, was the biggest clinical trial of AZT ever conducted: 1,749 patients over three years. It did not examine how effective AZT was in treating people who were seriously ill with Aids but, just as important, it looked at how effective the drug was in treating the millions of people with HIV, before they became unwell and showed Aids symptoms. Preliminary results of the trial were published in a letter in the Lancet, and made headlines worldwide. The results suggested that early intervention with AZT – for people who were HIV but had not yet developed any symptoms of Aids – was a waste of time. The study, organised by the British Medical Research Council and the equivalent body in France, reported that it made no difference to either mortality rates or disease progression if one took AZT before the onset of Aids.
In a ‘blind’ test, AZT was given to 877 people and 872 were given a placebo. As soon as a patient developed any Aids symptoms, he or she (15 per cent were women) would be offered ‘open-label’ AZT. The mortality rates appeared to be shocking: over the three years of the trial, there were 79 Aids-related deaths in the AZT group, but only 67 in the placebo group. The researchers explained that among so many patients this figure was not statistically significant, but if you were HIV-positive and read of this in the newspapers, you were bound to question all the great claims that had been made for AZT. More people got Aids and died on Concorde than on any previous trial.
There were other causes for concern. Those on AZT developed more side-effects than those on the placebo. The results of the tests also cast doubt on one of the fundamental ways we measure a person’s immunity to disease. Those given AZT early increased their ‘CD4’ or ‘T4’ cell count; these are the cells attacked by HIV, and their numbers drop as the disease spreads. But the fact that, even with this higher count, patients did not live longer or develop the disease more slowly, struck at one of the basic tenets of Aids research.
Cottrell told the news to his 28-year-old partner Karl Burge, who had been diagnosed as HIV-positive four years ago, and they decided to take action. But what could they do? They had already joined protests against Wellcome plc, the British company that made AZT and had reaped millions in sales and share profits. Wellcome executives had listened to their complaints, and had admitted to certain levels of toxicity in AZT, but claimed that their product still had great beneficial effects. They were not readily going to halt production of the drug that last year made them pounds 213m, their second biggest earner.
So Cottrell and his friends selected a new target, the Terrence Higgins Trust. This was a strange choice: the trust, Britain’s most prominent Aids charity over the past 10 years, is staffed by dedicated professionals and volunteers providing a large range of support and information about all aspects of Aids and HIV; it developed the caring ‘buddy’ system; it produced information for schools; it sat on many Aids research panels and often met government departments.
So what had it done wrong? It had taken money from Wellcome plc and included positive information about AZT in its many leaflets and documents. Cottrell and his friends felt they were being betrayed by the very organisation that they had believed existed to act in their best interests; they felt that what was once an invaluable institution was acting as a mouthpiece for a multinational pharmaceuticals company.
Last week, Cottrell and Burge were still pitched outside the Terrence Higgins Trust office in central London, four weeks after their protest began. On Wednesday they were arrested and charged with a public order offence after a member of the trust called the police. The protest is growing by the week. They have been joined by John Stevens, diagnosed HIV- positive more than eight years ago, and who also had bad experiences with AZT, and Pierre Hardy, diagnosed HIV-positive four years ago when he was 27 and had felt devastated by its effects. Many other protesters carry placards, collect signatures, hand out leaflets. You will not find a more potent symbol of the complex story of AZT, a story of how the struggle to find a ‘magic bullet’ to help millions of people has degenerated into a saga of distrust, confusion, and anger. It is a story of health and illness, but it is also a story of scientific ambition, secrecy and political pressure, and of the amounts of money that can be generated when a lethal virus turns into a worldwide epidemic.
IN 1964, Jerome Horwitz was working in his laboratory at the Michigan Cancer Foundation when he had what he hoped was a brilliant idea. At 45, Dr Horwitz was the foundation’s director of chemistry, and although not in the scientific premier league, was a respected local researcher with his own lab and assistants. He had spent much of the previous decade doing what many of the world’s leading scientists had done – working on a cure, or at the very least an effective treatment, for cancer.
He developed a theoretical solution: what was needed was a chemical that would insert a ‘phoney’ compound into the DNA ‘building block’ of a cell to prevent its replication. After years of research, Dr Horwitz came up with
azidothymidine (AZT).
He tried his new compound on leukaemic mice, but it had no effect. Horwitz didn’t know why, but AZT didn’t work.
Horwitz never became famous. Recently he said AZT ‘was a terrible disappointment . . . we dumped it on the junkpile. I didn’t keep the notebooks.’ The compound remained ‘on the shelf’, occasionally tried by other researchers but always found to be useless. There was no reason to patent it. But 20 years later, Burroughs Wellcome brought it back to life.
THE WELLCOME group was founded in London by two Americans in 1880. Its first significant achievement was the creation of the tablet – previously most medication had been administered in powder form. In the 1930s the group was split into two distinct parts: the Wellcome Trust, a large charity which devoted its income to scientific research and the maintenance of an institute and library concerned with the history of medicine; and the Wellcome Foundation Ltd, a profit-making pharmaceuticals company that was called Burroughs Wellcome in the United States. In the course of its research, Wellcome employees have won five Nobel prizes.
By 1980, Wellcome had specialised in the treatment of viruses for more than 15 years, and its anti-viral drugs accounted for the bulk of its income. In that year, David Barry, a leading researcher at Burroughs Wellcome in the US, noticed that demand for its drug Septra – a drug that Wellcome had helped to develop a few years earlier to combat a rare form of pneumonia – was suddenly on the increase. Previously this pneumonia, known as PCP, was prevalent only in children with leukaemia, but now many doctors were requesting it for adult males. Most of these men were gay, and living in New York and San Francisco.
Two years later, another new Wellcome drug, Zovirax, was in great demand among the same group of people. Zovirax was an anti- herpes treatment. Dr Barry was very disturbed by the sudden demand for these two drugs.
Aids (Acquired Immune Deficiency Syndrome) was first classified as a new disease in 1981, but it was not until 1984 that the cause was identified as HIV (Human Immunodeficiency Virus). This cause has since been challenged by several prominent molecular biologists, but it remains the cornerstone of Aids research. And if any company was ideally equipped to conduct research into combating a new virus, it was Wellcome.
It was only natural for Barry to devote much of the company’s research resources to fight HIV. No one knew how widespread the virus or Aids was or would become. In 1984, only about 3,000 people had been diagnosed with Aids, but some early forecasts were terrifying: millions of people might already be infected, and hundreds of thousands could die within the next few years. Any scientist could see that Aids was potentially a career-making race to the Nobel prize. Millions might be made from a successful treatment.
After a few years of government inactivity – shameful years in which this new disease was virtually ignored – political ambition added to the desire to find a treatment. Health departments noticed that it wasn’t just homosexuals who were being struck down, but also hundreds of haemophiliacs and drug users. A certain amount of official panic took hold: by the time Rock Hudson died in the summer of 1985, it was clear that anyone – even film stars – could be in the frontline.
According to Wellcome’s own three-page account, research into HIV began in June 1984. During mass testing of scores of anti-viral
compounds, a substance known at first only as Compound S was found to inhibit viruses in animal cells. Compound S was AZT, a resyn- thesised version of what Horwitz had made 20 years before (Wellcome credits Horwitz in its account, but spells his name wrong).
In November 1984, according to the Wellcome account, the company sent samples of AZT to Duke University in North Carolina, the Food and Drug Administration (FDA) and the National Cancer Institute for independent testing, and within a few weeks the results confirmed what Wellcome already believed: that the stuff worked against HIV in test-tubes under laboratory conditions. Wellcome had already progressed further than Horwitz, but the real test – its effect on humans – was fraught with danger.
But first there is another account of the development of AZT to consider. A US government official named Sam Broder believes he has far more claim to being ‘Mr AZT’ than anyone at Burroughs Wellcome. Broder, the director of the National Cancer Institute, claims that Burroughs Wellcome showed little interest in developing an anti-Aids drug.
Broder went on a tour of pharmaceuticals companies towards the end of 1984, imploring them to send any possible anti-viral compounds to his lab for testing in safe conditions. ‘I went to one prestigious company, hat in hand,’ he told the business writer Bruce Nussbaum, whose book, Good Intentions, traces a history of the search for anti-Aids drugs. ‘I got about one minute and thirty seconds of a high-ranking officer’s time. It was very disappointing for me. It was emblematic of the issue. There was no real interest in it.’
Broder then went to Burroughs Wellcome. He says: ‘They made it clear that on the basis of 3,000 patients, there was no way they could practically get involved.’ Broder says he then became abrasive. ‘As I left, I said, ‘You know, we’re going to have more than 3,000 cases. It is going to be commercially viable for you . . .’ ‘
Whoever pushed who, the drug came through. When Broder found that the AZT sent to him by Burroughs Wellcome in November 1984 worked against the virus, he assured the company that every effort would be made to get this great new drug to dying patients as soon as possible. The FDA’s stringent testing requirements mean that most new drugs take between eight and 10 years to pass from development to the marketplace. AZT was pushed through in just 20 months.
This could have been the early history of almost any drug; the difference is, during what would normally have been an eight-year test period, for six of those years the drug was already on the market. At a time of desperation, this drug looked like the one that would restore hope. The National Cancer Institute had previously tried one other therapy, Suramin, which proved to be toxic in early tests, but AZT appeared to be far less poisonous. And so it was put on the ‘fast track’: the testing of some other drugs for less life-threatening illnesses was put aside; AZT was given top priority, an all-or-bust thing. But could any drug live up to the boundless hopes pinned on AZT?
THIS IS how AZT is supposed to work against HIV. HIV enters body cells, usually T4 white blood cells that play a crucial role in the orchestration of the body’s immune system. HIV is one of a group of viruses known as retro- viruses, which means that, unlike most living things that store their genetic information as DNA, HIV stores it as RNA. Before HIV can replicate, it must convert its RNA code to DNA by use of a special enzyme. It is during this conversion process that AZT works. When AZT enters the body, it is transformed into a molecule that closely resembles one of the building blocks of DNA. During the process of HIV conversion, this molecule is incorporated mistakenly into the DNA. The addition of this ‘phoney’ molecule makes the addition of further building blocks impossible and halts replication of the virus. It’s a form of chemotherapy. It worked fine under a microscope.
The first human tests were in two phases. The first examined whether AZT could be tolerated in the body at all, and whether it entered the brain, crossing the ‘blood-brain barrier’; to know this was important, because a common Aids symptom is dementia. The first Aids patient was injected with AZT in July 1985. This test concluded that the blood-brain barrier was crossed, and that although there were levels of toxicity detected, these were deemed to be safe.
The second phase of the tests, the final hurdle to the granting of a licence for mass production, was a shambles. It was set up six months later to establish whether AZT would combat Aids. This test, overseen by the Food and Drug Administration, involved 282 patients, all of them already ill with Aids or Arc (Aids-related complex). It was to be a placebo test, conducted over 24 months. It was to be a ‘double-blind’ study in which neither patient nor doctor knew whether the capsules being taken were AZT or starch. (But before the tests could begin, Wellcome had to produce large quantities of AZT, and found it couldn’t do it. It had run out of one crucial ingredient: herring sperm. Finally, Wellcome bought it in bulk from another company.)
At a press conference after the tests in September 1986, Wellcome reported that they had been a considerable success, such a success that the 24-week trial had been halted after 16 weeks for ‘ethical’ reasons. Mortality rates for people taking AZT were staggeringly lower than those taking the placebo; there had been 19 deaths in the placebo group of 137 people, but only one in the AZT group of 145. Those on AZT also had a decreased number of opportunistic infections and showed improvement in weight gain and T4 cell counts. Wellcome agreed in response to pressure from some sectors of the gay community that if AZT was effective, then dying people should be taken off the placebo at once.
No one claimed it was a cure, but there was huge relief that a breakthrough had been made. There had been much embarrassment when it became known that Rock Hudson had attended the Pasteur Institute in France for treatment; now at last America was showing those foreigners a thing or two. Robert Windom, assistant health secretary, said that ‘treatment with AZT prolongs survival of persons with Aids’. The results were ‘exciting’.
It was not suitable for everyone, but it was the best thing yet. In fact, it was the only thing. Last year, interviewed in the Wellcome in- house magazine, David Barry said that ‘the staff at Wellcome can tell our children, grandchildren and great-grandchildren that we were there, that we made a difference’. When it was shown that AZT worked, ‘we . . . first had a frenzied, cheerful celebration, and then a very quiet one. The longer we considered the global implications, the greater the accomplishment we realised Wellcome had made in the control of the HIV epidemic.’
But a few months after AZT was made available, John Lauritsen, a journalist working on the gay newspaper New York Native, obtained test documents through the Freedom of Information Act that suggested that many rules had been broken in the trials. The trial had been ‘unblinded’ within weeks: some patients claimed they could tell what they were taking by taste; others were so keen to have AZT that they pooled their treatment with other patients to increase their chances of receiving the drug. The documents showed that almost half the AZT patients had received numerous blood transfusions in the course of the trial, because of damage to their bone marrow and immune systems; and that a few had to be taken off AZT altogether.
What happened after the trial ended suggested something more alarming about AZT. After 16 weeks, one AZT patient was dead, compared to 19 placebo patients; a week later two more patients on AZT had died, compared to four more on the placebo. The ratio had switched from 19:1 to 23:3, which suggested AZT might only be effective for a limited time.
If the trial had continued, the ratio might have narrowed even more. The tests would probably still have shown that AZT has some benefits for very ill patients, but with hindsight it is alarming that a new drug was allowed to be
released with so much left to prove. People at Wellcome now put it down to the mood and the severe pressure of the times. Dr Trevor Jones, Director of Research at Wellcome, who has been involved in their development of AZT from the beginning, acknowledged that the trials were subject to extraordinary pressures. ‘Much of these accusations (about the breakdown of trial protocol) took place, not at that stage, but later on, when the drug was showing benefit in a less sick population.
All sorts of things we heard stories about, and some of them I think we can confirm from our data. Patients would go to their doctor, get their treatments, and rather than risk the uncertainty (or receiving the placebo), they’d put the two together, mix them and divide them by half. We know this, because people who were supposed to be on the placebo already had drug levels in them.’
Much of the pressure came from people with HIV and Aids, and their carers, who wanted the drug released immediately. It was unacceptable to administer a placebo, they argued, if AZT worked. And there was no point having a drug released on the market in 10 years – by that time hundreds of thousands would be dead.
Burroughs Wellcome and many other independent research institutions would spend every subsequent year trying to supplement their data on AZT, trying to find out all the things that would normally be known about a drug before it hit the market. In these later years AZT was to become for many people the symbol of all that was wrong with Aids research. Once AZT was shown to have worked, almost all available funds were channelled to support its development and other potential treatments, along with any doubts that HIV was the cause of Aids, were swept aside.
BUT IN 1986, AZT was unstoppable. It suited the FDA, because it showed the administration was doing something. It suited Wellcome, because it now had a patent on AZT (and by 1986, with the epidemic increasing alarmingly, there was no doubt that the financial rewards would be enormous). It suited doctors, because they believed they could help their patients. And it certainly suited people with Aids. Some people had doubts, but hell, if you were ill and dying you wanted to believe. After all the despair and uncertainty, people in authority were saying ‘take this, it’ll do you good’.
Cottrell was one of the first people to take AZT in Britain. He was prescribed it in 1986, before it was widely available, when he was 23.
‘I had recently been diagnosed HIV-positive, and I went into a panic. I thought I was going to die. I remembered something about this drug coming from America and everyone clamouring to get it. I was perfectly healthy. My boyfriend’s blood count was quite low, and he was prescribed it by St Stephen’s Hospital, and I took it too. Intuitively, I didn’t think it was doing me any good. I was prescribed it three times over a period of three years, and I took it out of fear. I was first prescribed 1,200mg a day, and then 500mg, but I still felt bad, even on the lower dose. I had nausea and headaches and muscle fatigue.’
Cottrell took it every four hours, which meant he had to have a bleeper that woke him at three or four o’clock every morning. (People joked that the real Aids money lay in making these bleepers; in New York in the late Eighties, opera performances were punctuated by bleeps.) Cottrell stopped taking AZT after a few weeks, but then he got scared, and began taking it once more. ‘I got my drugs every two weeks – a big plastic bagful. I felt that I was carrying my life around in that bag.’
His friend, Pierre Hardy, was diagnosed HIV in 1989, when he was 28. At a specialist clinic he was given a sheet of paper which explained that AZT was the most efficient treatment, but also that it hadn’t been around long enough for anyone to know the long-term effects. Like most people in his position, he said he’d try anything, and he was prescribed 500mg a day.
‘My T4 count went up along with my general health in the first year, and everything settled down. I had been on AZT for three years, and my T4 count was levelling between 400 and 600 (an average T4 count in healthy adults is between 800 and 1,000). And then last year I started to get sick. I had repeated chest infections, and in November 1992 I had a stroke. I was hospitalised in a specialist ward. I asked them for my T4 count, and when they came back, they were were uncomfortable about it. My T4 count was 90. I thought I was finished.
‘When I got home and started to review the whole thing, the whole HIV theory. I threw away all the pills I was taking – I was taking seven every morning and evening. I started to change my diet, and then I went back to my doctor. When I had my new T4 count it was 545. I’ve had three migraines since January, a little bit of asthma coming back, but basically I feel much better. If I’d continued to believe in the traditional medicine sytem I would have been dead either this year or next year.’
Two weeks ago Hardy met a volunteer with the Terrence Higgins Trust, who told him that he and his boyfriend were taking AZT and it was working like a dream.
‘I asked him how long they were on it. He said four months. I said that that was the trap that everyone was falling into. The AZT will work for you for a little while, for the maximum of one year, as it did for me, and afterwards the damage became visible.’
Most people with Aids, and many with asymptomatic HIV, take or have taken AZT. Other drugs have emerged in the past few years that work in a similar way – DDC (produced by the Swiss company Hoffmann-La Roche) and DDI (made by the American company Bristol-Myers Squibb), but AZT is still the market leader. It is hard to think of another product that is so dominant in its field. You read the showbiz autobiographies and those three little letters snap out of the page.
Earvin ‘Magic’ Johnson, the basketball star who tested HIV-positive in October 1991, was advised to take AZT immediately. He agreed. ‘There was a lot of public interest in the fact that I was taking AZT, which was originally used only in the later stages of the illness,’ he explained in My Life, his autobiography. ‘These days it’s used as a preventative, but not everybody knew that. That may be why some people, including a few reporters, concluded that I was sicker than I actually was.’ People wrote to Johnson telling him that AZT was not the answer. Somebody advised him to drink all his blood and replace it with new blood. ‘Even now I can’t go anywhere without somebody coming up and saying, ‘I know this friend who knows this doctor who has a cure’.’
Rudolf Nureyev, who died in January, began taking AZT in 1988. ‘AZT was just beginning to be used in France,’ said Michel Canesi, his doctor. ‘I didn’t want to give it to him straight away, because I was worried that the side-effects would hamper him (Nureyev was still dancing at this time). Rudi lost his temper and said: ‘I want this medicine.’ I replied that there hadn’t been long enough to judge the results. But I had to give in and prescribe it – he was so insistent. But he didn’t take it regularly. He went off every time with tons of drugs, and every time I went to see him I found unused packets all over the place.’
The film-maker Derek Jarman, who was diagnosed HIV-positive in 1986, has found AZT beneficial. ‘It works – it holds everything up. It stops the virus replicating. At the beginning they gave people much too massive doses, which affected us physically. I had no recognisable toxic side-effects from it. I began taking it in September 1990, I think, and I came off it last August.
‘I was invited by my doctor to make up my mind whether I took the drug or not, so I rang up various people in America and the general advice was to take it – and this was advice was from quite radical people, not people in with the Wellcome Foundation.
‘I came off it because my doctor said that my (T4) count was down. We’ve never discussed it since. He just suddenly said, ‘I think you’ve had enough AZT, Derek’, and I very much trust him, he’s a brilliant doctor. The whole thing is so complicated, because I took a lot of other drugs as well. I had to have suppressants for TB, toxoplasmosis and PCP. And then obviously if I got an infection there was fluconazole and all of that area. And then at a certain point they added hydrocortisone and fludrocortisone to keep my energy up.’
Jarman has recently been in hospital. ‘At the moment I’m actually on nothing. I’ve had a skin complaint and they decided it would be very sensible to take me off all my pills, and then go back on the drugs to see if they were causing the skin complaint. They can obviously play around with the drugs.
‘My feeling about AZT is that I’m glad I took it, even though I can’t prove to you that it did anything. You can say that if it helps someone psychologically then it must be doing some good. I think the doctors generally feel that it does some good. But how do you know?’
FINANCIALLY, Wellcome plc has done extremely well out of AZT. Retrovir, the drug’s brand name, accounts for more than 13 per cent of its total income, and yielded pounds 213m last year. As the only big earner to have been launched by the company in the past decade, the continued success of AZT is crucial to its growth. The company will be well aware that at the end of last year the World Health Organisation estimated that about 13 million men, women and children have been infected with HIV since the start of the pandemic. (A large proportion of these cases are in sub-Saharan Africa and South and South-east Asia, where AZT and other anti-Aids treatments are unlikely to be available or affordable; the figure for HIV infection in the Americas and Western Europe is estimated at 2.5 million.)
Part of the Wellcome Foundation was floated on the stock market in 1986, the year of the AZT breakthrough. Subsequent rises in share prices have been directly linked to the fortunes of the drug and the results of new trials. In February 1987, the share price jumped 73.5p to 374.5p on the news that AZT would be widely available in the US at dollars 188 for 100 capsules, an extremely high price for a new drug, and one that would yield large profits (this translated to about dollars 10,000 a year for every user). By November 1989 the share price had almost doubled to 724p; year-on-year pre-tax profits were up 28 per cent to pounds 283m. In early 1993, the share price was at 810p; last year’s pre-tax profits were pounds 505m.
‘In terms of the emotive quality of the demand, there’s never been a drug like it,’ said Martin Sherwood, a Wellcome spokesman, shortly after AZT’s launch. It was just this emotive demand that led to the picketing of the Wellcome shareholders’ meeting in January 1990. Act Up (the Aids Coalition to Unleash Power, co-founded by the playwright Larry Kramer) picketed the AGM at Grosvenor House in London, describing it as ‘a gathering of Aids profiteers’. Activists complained about the price of AZT, and what they saw as Wellcome’s reluctance to provide all available information on the drug.
Wellcome shareholders were irritated by this intrusion, not least when Act Up members interrupted the meeting and insisted on talking to Sir Alfred Shepperd, the outgoing chairman. But Wellcome executives were baffled: they believed they had done everything they could to benefit people with HIV and Aids, certainly more than any other pharmaceuticals company. Was it not these very same activists who had celebrated when AZT was launched three years earlier? At first Wellcome defended its pricing on the grounds that AZT took dollars 80m to develop and produce (later revised to dollars 30m), but it soon bowed to pressure (and its economies of scale) and cut the price. The recommended dosage was also reduced for medical reasons, which meant many more people could tolerate its toxicity. Today AZT costs about dollars 3,000 per person per year, or about pounds 2,000.
As would be expected, Wellcome plays up the good news. When, in 1989, two double- blind placebo trials of the effects of AZT on asymptomatic and less seriously ill patients showed that it could delay the progression of the disease, much was made of the results and the share price rose by 30p. But when, four months later, the company admitted that AZT had caused cancer in rodents, it explained that the rats and mice were given 10 times the dose prescribed to humans, and that several other drugs in use by humans had also produced tumours in animals when administered over long periods. Wellcome’s share price went down one penny.
Wellcome’s PR machine is an impressive force, and much money is spent on convincing the media of AZT’s worth. You go and see them and you get a lot of bumph: how AZT works, why it is more effective than other anti- retrovirals. Wellcome house-magazines talk of the extra 400,000 productive years of life it has made possible through the drug, about how many thorough and independent studies have stressed AZT’s efficacy.
‘The number of people who have shown agression against us concerns us no end,’ says Trevor Jones. ‘Normally the company tries to distance itself from the patient / physician interaction – it must do. The day-to-day therapy of the patient is not our responsibility. But about three years ago we started to open our labs to people with HIV and their carers, contrary to the advice of my security and other colleagues. You then realise the uncertainty and the frustrations involved in that act of taking a tablet for the very first time. When people with HIV came through the door of the lab I could almost touch their anger. But I realised that the anger was not really about Wellcome or me, but about their mortality. They were frustrated, and saying, ‘Please, please what can I do?’ These were genuine cris de coeur.’
Dr Jones is one of the few pharmaceutical industry representatives on Britain’s Medical Controls Agency. Wellcome has clearly selected its spokesman with care. ‘People say we’re purely acting out of commercial interests, but it is not in our commercial interests to do anything else but get this drug right,’ Dr Jones says. ‘We wanted to show people that we are working night and day, weekdays and weekends trying to develop better medicines. Otherwise we look like ogres and robber barons all the time. That’s the whole history of our business; if you’ve got a problem with a product, you must, you must, you must tell people. The criticism hurts a lot; our integrity as a scientific body is important to us. I don’t take too kindly to people saying, ‘Oh, you don’t want to listen to Wellcome, because they would say that, wouldn’t they?’ You can’t hide anything in this business, because otherwise who will trust us when we develop another drug, like the new epilepsy drug we’ve got now? You have to believe that the integrity of science is good.’
Jones has had a bad few weeks. Wellcome’s share price was hammered by last month’s Concorde trial report, falling 10 per cent to 670p, before rallying to 692p. Five days after the report appeared, Wellcome staged a damage limitation exercise, at which Jones told a press conference that he was unhappy with the way the results were released, without peer review or advice to patients, and saying it had caused panic among those with HIV. He said that the full results had yet to be released, and hoped that a more beneficial picture of early intervention with AZT would emerge at the ninth International Aids Conference in Berlin in June. He also outlined that the protocol of the study had changed from that agreed in 1988. When an American study reported in 1989 that AZT did have beneficial effects on people with asymptomatic HIV, the Concorde officials decided that people on its trial could switch to AZT if they wanted to; this may have led to a diluting of the results.
Last week, Jones reiterated why AZT may still be beneficial, and why doctors should continue to prescribe the drug early. ‘We have gathered together 10 studies on asymptomatic patients. Five of these are control studies with placebos, and five are cohort studies, in which we simply give the drug and observe what happens. These studies involved more than 6,500 patients and ranged from one to four years in duration. We believe we have accrued sufficient data to show that taking the drug when you’re asymptomatic does delay the onset of further symptoms.’
WELLCOME has a presence at all the chief Aids conferences, and will occasionally organise gatherings of its own. In June 1992 it launched Positive Action, ‘an international intiative’ in support of those with HIV and Aids. For the launch conference in London, journalists flew in from all over Europe to hear Wellcome executives describe how pounds 1m was being distributed to many educational organisations. An emotional climax of sorts was provided by Jerry Breitman, the company’s US director of professional relations. He was there to present the ‘workplace initiative’, and his speech contained a little surprise at the end. Like the wig salesman whose coup de grace is to rip off his own toupee, Breitman declared himself HIV-positive. ‘I thought long and hard before deciding to tell my management,’ he revealed. ‘But . . . when you are part of an enlightened organisation such as Wellcome, I am absolutely convinced that communicating your HIV infection is a positive action . . . It is, truly, one of the best decisions I have made in a very long time.’ A few journalists felt distinctly queasy at the theatricality of it all.
One of the initiatives raised was Wellcome’s involvement with the Terrence Higgins Trust. This first surfaced in 1991, with the publication of four information leaflets. Two months ago staff at the Trust and volunteers read in their newsletter that the link had been strengthened. The newsletter explained that ‘THT, along with the Wellcome Foundation, is about to begin producing an important new medical information series. THT are providing a series of medical updates for all staff and volunteers. We will be providing them on a regular basis every two months in the evening. Costs will be met by the Wellcome Foundation, which also funds our series of general booklets.’
Nick Partridge, chief executive of the trust, is dubbed ‘Nick the Sick’ on the placards carried by the protesters outside his office. Partridge, in reply, calls them ‘New Age flat- earthers who have a naive hope that Holland & Barrett will produce a herbal tea that will be effective against HIV.’ Partridge said that the trust actively pursued funding from a wide range of companies and government agencies, and that it was ‘quite clear that none of that funding involves an ability by those companies to influence the information we produce. We would be neglecting our duty if we were not in regular contact with Wellcome, Bristol-Myers Squibb and Roche, arguing for greater investment in HIV research and fair and balanced information. The leaflets are not about treatment issues.’
But once they were. In 1991 the trust produced a 24-page booklet on HIV and its treatment; nine pages were devoted to AZT, but only half a page was given to other therapies. The copyright on the leaflet was held by the Wellcome Foundation, which also paid for its printing. ‘It was only available for eight months,’ Partridge says. ‘Information changes quite rapidly. The main fault of that leaflet is that it is too hopeful. By 1991 the hopes around early intervention had probably gone further than we realise, in retrospect, was wise. The desire by many people with HIV to say, ‘Yes, we can live with this infection’ meant that a lot of hope was invested in the theory of early intervention. For all its faults, our leaflet was still a lot more realistic than the material that Wellcome was putting out on its own. Remember that over the years, there have been many stories of breakthroughs that proved to be wildly optimistic.’
FOR MOST people with HIV, the AZT dream is over. AZT is the future that was; no one believes in the ‘magic bullet’ any more. It does have benefits for some patients who are seriously ill, but there is now severe doubt over its other uses. This, after the drug has been subjected to more tests, and has been the subject of more post-launch research papers, than perhaps any other modern therapy.
The future for HIV and Aids treatment appears to be in combination treatment – the use of AZT and DDC and DDI and many other compounds used in all manner of variations. Several trials are in progress. Two weeks ago it was announced that Wellcome has joined forces with its competitors Hoffman-La Roche, Bristol-Myers Squibb, Glaxo, SmithKline Beecham and 15 other companies, in an attempt to pool their research knowledge and find an effective treatment.
Wellcome is also developing some other anti-Aids drugs on its own. We won’t hear about these for a while; the company doesn’t want to raise any hopes.
Jerome Horwitz, the man who created AZT in 1964, is still active in medical research. He’s 74 now, but you can still reach him most days at the Meyer L Prentis Cancer Center in Detroit. Occasionally he does a little Aids work, but most of his time involves cancer chemotherapy.
Horwitz believes AZT is not the answer to HIV and Aids, but has hopes for combination therapies (he was also the first to synthesise DDC). He concludes that AZT ‘buys time’.
‘We were certainly on the cutting edge,’ he says of his work in the mid-Sixties. ‘When the pharmacologist said, ‘Look, Dr Horwitz, your compounds are not effective against leukaemias and I see no future for them’, that was like a blow to the solar plexus. We had great hopes. ‘I remember one of my students saying at the time that we had a great series ofcompounds just waiting for a disease totreat. It took 25 years before our beliefs were vindicated.’
The first Horwitz heard of AZT’s use against HIV was when he read about it in the Wall Street Journal. Burroughs Wellcome established a chair in his name at the Michigan Cancer Foundation, but he has received no financial reward.
‘My wife sits across from me at the
breakfast table and reminds me of all the
money that Burroughs Wellcome has got out of it and I haven’t got a dime. I keep telling her about the legacy I’m leaving. But I wouldn’t be being absolutely straight with you if I hadn’t thought that I should have gotten something out of it.’-
Nothing raises my hackles more than watching any documentary on ex-gay conversion therapy! It is bad enough when adults submit themselves to this degrading process, brought about almost inevitably by peer and social pressure. However, when parents send their below age-of-consent children to places like a Love In Action/Refuge conversion therapies, one really has to wonder just how shallow parental love can be! These so-called ex-gay conversion therapies by a whole range of organisations that fell under the Exodus International umbrelladisplay everything that is wrong, and evil, about Christianity: hypocrisy, prejudice, discrimination, stigma, deceit, misinformation, guilt, manipulation, and out-and-out lies to force an antiquated system of belief on teenagers at a difficult and confusing time of their lives, a time where personalities and sexuality are running rampant through rapidly changing bodies. We know, for a fact, that gay people cannot be turned straight. You’ve just gotta love how some of these ‘ex-gay” members love to flaunt their wives, kids and marriages as proof that the therapies work! Denial can be a strong motivator in some people’s lives. Both the 30% suicide rate amongst ex-gay conversions…probably motivated by the so-called therapy apparently not working…and that there are ex-ex-gay groups for those who attended therapy sessions and yet still found themselves with gay inclinations would seem to say all that needs to be said about the high failure rate of conversion therapy.
Obama’s call to ban the practice reflects a tectonic shift within the community that once championed it.
ANDREW KELLY/REUTERS
Throughout the 1980s and 90s, the Christian right poured money and muscle into promoting the message that homosexuality was a curable disorder. It advocated conversion therapy, which promised to turn gay men and women straight. But last week, when President Obama announced his support for a national ban on such therapies, few voices on the Christian right spoke up in protest. The announcement confirmed the evaporation of support for these approaches among the communities that once embraced them. As Alan Chambers, who once ran America’s largest ex-gay ministry, told me, “sexual orientation doesn’t change.”
It was a shift rooted in the accrual of evidence and experience. After she came out as a lesbian in high school, Julie Rodgers’ conservative Christian parents urged her to join a ministry in Texas to help make her straight. Ministry leaders promised her that if she continued praying, reading the Bible, attending meetings, and of course, refusing to identify as gay, her sexual orientation would eventually change and she could even marry a man. Rodgers didn’t want to go, but she did want the food, shelter, and love her parents offered. So she agreed.
The program worked great—except that it didn’t. After a decade of compliance, neither Rodger’s orientation nor those of her fellow group members budged toward straightness. And worse, the empty promises and feeling that she was “less than” normal left her drowning in a sea of shame.
It’s a sad story, but one that grows gloomier when you consider that Rodgers is one of the lucky ones. Countless LGBT youths have been subjected to much worse, not just in Christian ministries, but also at the hands of licensed counselors who perform what is known as “reparative” or “conversion therapy.” These controversial mental health practices, intended to change a person’s sexual orientation or gender identity, are ineffective and often drive participants to depression, anxiety, drug use, or suicide.
In recent years, however, conversion therapy has been much maligned if not completely discredited. Almost all major medical and public welfare organizations oppose it, and even conservative Christians—once counted among its strongest supporters—are changing their minds. New Jersey, California, and Washington, D.C., have already outlawed ex-gay therapy for minors. By all accounts, therapies attempting to cure gayness appear to be going the way of the buggy whip.
But this hasn’t always been so. According to Kenneth Lewes, in his book, Psychoanalysis and Male Homosexuality, some began to view same-sex erotic behavior less as sin than as a mental-health disorder as early as the 19th century. This was true of other “sinful” behaviors as well—for example, drunkenness morphed into alcoholism and demon possession became schizophrenia or a personality disorder.
The shift was spurred on by the work of Sigmund Freud in the early 1900s, even though the iconic neurologist was pessimistic about either the possibility or desirability of changing homosexual orientation to heterosexual. Freud’s belief that human beings are born bisexual and can move along a continuum of sexuality formed the basis of the belief that homosexuals could be “cured.”
This way of thinking about sexual orientation persisted into the mid-20th century as many Americans fantasized about an idyllic “traditional family” in the Father Knows Best and Leave it to Beaver molds. By the start of the American cultural revolution in the 1960s, many mental-health professionals, clergy, and politicians supported the idea that homosexuality was a mental-health disorder that could be cured through some combination of prayer and “therapy,” which included electroshock therapy, masturbatory reconditioning, and giving patients nausea-inducing drugs while forcing them to view homosexual erotica.
“One reason why homosexuals are so rarely cured is that they rarely try treatment,” proclaimed a 1965 Time magazine article. “Too many of them actually believe that they are happy and satisfied the way they are.”
But the late 60s and 70s brought on a blitzkrieg of social change. Women’s liberationists energized the feminist movement, the conflict in Vietnam provoked an anti-war movement, a growing awareness of ecological degradation brought on the environmental movement, and an increasingly mobilized LGBT community morphed into a powerful gay-rights movement.
In 1974, the American Psychiatric Association voted to remove homosexuality from its list of mental health disorders. This inflamed many conservatives, especially the Christians among them, who were now mobilizing in the public square against what they believed was a growing tumor of secularism.
Christian pastors promoted anti-gay messages from their pulpits, even advocating the idea that HIV/AIDs was a special form of God’s wrath and judgment against human sinfulness. Christian funders helped bankroll ex-gay ministries like Exodus International, which grew into a coalition of more than 80 ministry partners across 34 states. In 1998, Christian political groups even spent $600,000 on pro-conversion therapy ads in The New York Times, USA Today, The Wall Street Journal, Los Angeles Times, and other publications. Robert Knight of the Family Research Council called it “the Normandy landing in the culture war.”
As a result, ex-gay therapy experienced something of a resurgence in the 1990s. Newspapers often treated it as a medically viable option, and Newsweek ran a sympathetic cover story in 1998.
But the foundations of this effort began crumbling at the turn of the 21st century. While peer-reviewed evidence for the efficacy of aversive therapies was lacking, a growing body of scientific studies indicated that it was not effective in altering subjects’ sexual orientations and was potentially harmful. (The main study cited in support of conversion therapy was conducted by Robert L. Spitzer, who later apologized and admitted his data was tainted, unreliable, and misinterpreted.) After reviewing such studies, major medical organizations—the American Medical Association, American Academy of Pediatrics, American Counseling Organization, National Association of Social Workers, World Health Organization, and others—systematically repudiated these practices as harmful.
While science was discrediting conversion therapy, high-profile ex-gay leaders were either apologizing and defecting to the other side or being exposed as frauds. John Paulk, a man who had been a vocal and visible supporter of gay conversion for more than a decade and claimed to be happily married to a former lesbian, was photographed in a Washington, D.C., gay bar in 2000. Three years later, it was discovered that Michael Johnston, founder of “National Coming Out of Homosexuality Day,” was having unprotected sex with men he’d met online despite being HIV-positive. In 2006, Ted Haggard, a fiery opponent of gay rights and then president of the National Association of Evangelicals, admitted to having gay sex with a male prostitute after unsuccessful attempts to change his orientation through counseling. A few years later, John Smid, former executive director of the ex-gay advocacy group “Love in Action,” apologized and said he “never met a man who experienced a change from homosexual to heterosexual.” These names are only a sampling.
By the second decade of the 21st century, the scientific foundation of reparative therapy had eroded, every major medical association had repudiated it, the movement’s leaders were falling away, and viral horror stories from former participants were popping up across the web.
But the death-knell sounded in July of 2013 when Alan Chambers, president of Exodus International, America’s largest ex-gay Christian ministry apologized to the LGBT community and shuttered his organization. Chambers once claimed he knew “tens of thousands of people who have successfully changed their sexual orientation.” But last week, he told me “99.9 percent of people I met through Exodus’ ministries had not experienced a change in orientation.”
Chambers’ announcement seemed to unleash a broader shift among conservative Christians, the last defense against reparative therapy’s demise. Julie Rodgers, the ex-gay ministry survivor from Texas, now serves on the ministry staff at Wheaton College, one of America’s most prominent evangelical universities, where she has spoken against ex-gay therapy. Russell Moore, the political pointman for the Southern Baptist Convention, has publicly repudiated the practice. Even the opinion editor at the school newspaper for Liberty University, founded by the late Jerry Falwell, editorialized against it.
In 2011—roughly half a century from gay conversion therapy’s heyday—only 24 percent of Americans said they believe it works. The number is presumably even lower today.
While some disparate pockets of support remain, they are waning. The day when ex-gay therapy enjoyed legitimacy in mainstream medicine, media, religion and society is now heading for the history books. And in its place, there is a growing consensus that such practices are distasteful, irresponsible, unethical—and perhaps should be illegal.
Religious Faith Linked To Suicidal Behaviour In LGBQ Adults
(Reuters Health) – Although religiosity is generally tied to reduced suicide risk, the opposite may be true for some young lesbian, gay and questioning adults, researchers say.
Based on data from more than 21,000 U.S. college students, researchers found that greater religious feeling and engagement was tied to increased risk of suicidal thoughts and actions for participants who identified as LGBQ.
“Religion has typically been seen as something that would protect somebody from thoughts of suicide or trying to kill themselves, and in our study our evidence suggests that may not be the case for everyone, particularly for those we refer to as sexual minority people,” said one of the study authors, John Blosnich of the Injury Control Research Center at West Virginia University in Morgantown.
Previous research suggests that belonging to a religious faith reduces risky behavior in young people, such as substance use and unsafe sex, Blosnich noted in a telephone interview. Religiosity has also been linked to a lower risk of suicidal behaviors, but there is some evidence to suggest that the impact of religion may be different for lesbian, gay, bisexual and questioning (LGBQ) individuals.
The study team analyzed survey data from the 2011 University of Texas at Austin’s Research Consortium on 21,247 college-enrolled 18- to 30-year-olds, including 2.3 percent who reported being lesbian or gay, 3.3 percent who identified as bisexual and 1.1 percent who were questioning their sexuality.
All participants rated the importance of religion in their lives on a 1 to 5 scale, from “not important” to “very important.” Between 21 percent and 28 percent of LGBQ participants rated the importance of religion to them at a 4 or 5, compared with 39 percent of heterosexuals, researchers report in American Journal of Preventive Medicine.
Questioning youth had the highest rate of recent thoughts about suicide, at 16.4 percent, compared with 3.7 percent of heterosexuals, 6.5 percent of lesbian/gay individuals and 11.4 percent of bisexuals. Lifetime suicide attempts were reported by 20 percent of bisexual youth, 17 percent of questioning youth, 14 percent of gay or lesbian youth and 5 percent of heterosexuals.
For bisexual youth, the importance of religion was not associated with suicidal behavior, while religiosity was protective against thoughts of suicide and suicidal attempts in the heterosexual youth. But lesbians and gays who reported that religion was important to them were 38 percent more likely to have had recent suicidal thoughts. For lesbians only, religion was associated with a 52 percent increased likelihood of suicidal thinking.
Questioning individuals were almost three times as likely to have attempted suicide recently if they reported that religion was very important to them.
Among lesbians and gays who said religion was not important to them, there was no association between sexual orientation and recent suicide attempts. But being homosexual did significantly increase the likelihood of recent suicide attempts in people who said that religion was very important to them.
“Some sexual minority folks are really at odds. They feel very confused or they feel that they are in conflict with their faith because of who they are. That’s a very scary place to be in,” Blosnich said.
“We are definitely not saying that religion, period, is bad; it’s not,” he added. “There are many sexual minority people who find great strength and great sources of support in their religious communities, but unfortunately we hear many stories about people who do not.”
Faith-based partners in public health suicide prevention and intervention services “should be willing and equipped to assist all people who seek their services, regardless of sexual orientation,” the study authors write.
atizing views of sexual minorities, the authors note. Because the study population was drawn from an academic setting, it may not represent the general population, they add.
“We want to engage religious and faith-based providers in a way that benefits all people,” Blosnich said. “Faith-based communities are major participants in suicide prevention. We just want to make sure that the services that people provide through faith-based organizations or through community faith partners reach everyone who comes to them for help, regardless of sexual orientation.”
SOURCE: bit.ly/2qt3gYC American Journal of Preventive Medicine, online March 15, 2018.
Former Love In Action Leader Marries His Same-Sex Partner
John Smid, the former director of Memphis-based ex-gay ministry Love In Action, has announced his marriage to partner Larry McQueen. The two married in Oklahoma on Sunday, November 16th.
Smid has been living as an out gay man for several years now, and he’s been in a relationship with McQueen for one year. Gay marriage just became legal in Oklahoma last month. The couple live in Paris, Texas, where Smid moved from his Memphis home in the summer of 2013.
Smid’s journey from ex-gay leader to happily out gay man has been a long one. He was promoted to the role of executive director of Love in Action in September 1990, and in 1994, the organization moved its ministry to Memphis. Love in Action operated here quietly until 2005, when protests over a youth “straight” camp called Refuge sparked a national media firestorm.
In early June 2005, Zach Stark, a White Station High School student, posted these words on his MySpace page: “Today, my mother, father, and I had a very long ‘talk’ in my room, where they let me know I am to apply for a fundamentalist Christian program for gays.”
That fundamentalist program, described by Stark in a later post as a “boot camp,” was Refuge, a two-week day camp where gay kids were taught how to become straight kids. After Stark’s MySpace post, local LGBT equality advocates held a week of protests outside Love In Action, and the Memphis ministry made national headlines, including a story in The New York Times.
Love In Action eventually discontinued the Refuge program and moved to an adults-only conversion therapy model. All the while, Smid was struggling with his own beliefs. During the week of protests in 2005, Smid met Memphis filmmaker Morgan Jon Fox, who was working on a documentary about Love In Action. Smid told the Flyer in a previous interview that it was Fox’s influence that helped open his eyes to the fact that conversion therapy was doing more harm than good.
“As we got together, we were willing to lay aside our agenda and get to know one another as people,” Smid said of Fox. “That was very instrumental in my processing where I am today.”
Smid eventually resigned as director of Love In Action in 2008, and he founded Grace Rivers, a monthly fellowship for gay Christians. At the time, he remained married to his wife. But they eventually divorced in 2011. Earlier this year, Smid told The Lone Star Q, a Texas LGBT news organization, that he couldn’t continue living the rest of his life in a marriage that didn’t feel right.
“I’ve believed in faith that something was going to happen, and it never did, and so at my age, right now in my life, I don’t have that many good years left in me, and I can’t live like this for the rest of my life, so I said no I’m not willing to keep pushing after something that’s not going to happen,” Smid told The Lone Star Q, regarding his divorce.
Smid met McQueen three years ago, but they were just “acquaintances with common friends,” wrote Smid in his Facebook announcement of their marriage Sunday.
“I gradually got to know him over time until we reached a place in our lives that we saw we wanted to get to know one another through a dating relationship. As we dated we shared our vision for life, our personal philosophies, and our faith values. We found a compatibility that was comfortable and exciting,” Smid said.
He went on to say, “I realized this week that my relationship with Larry is a mirror I see in every day. For most of my life, the mirror I saw reflected my mistakes, shortcomings, and failures. The reflection I see today with Larry shows me the positive things in my life, my strengths, gifts, and talents. I see how I can succeed at a mutual intimate and loving relationship. For this, I am truly grateful.”
Ex-Gay Group Exodus International Shuts Down, President Apologises
Exodus International, a group that bills itself as “the oldest and largest Christian ministry dealing with faith and homosexuality,” announced June 19 that it’s shutting its doors.
Exodus’s board unanimously agreed to close the ministry and begin a separate one, though details about the new ministry were unavailable at the time of the organization’s press release.
The announcement came just after Exodus president Alan Chambers released a statement apologizing to the gay community for many actions, including the organization’s promotion of efforts to change a person’s sexual orientation.
“I am sorry we promoted sexual orientation change efforts and reparative theories about sexual orientation that stigmatized parents,” Chambers said. “I am sorry that there were times I didn’t stand up to people publicly ‘on my side’ who called you names like sodomite—or worse.”
The announcement comes at a critical point for gay rights, as the U.S. Supreme Court prepares to issue two potentially decisive rulings on gay marriage and public opinion shifts rapidly in favor of gay rights and even gay marriage.
A recent Gallup Poll showed that 59 percent of Americans now view gay or lesbian relations as “morally acceptable,” a 19-point swing since 2001 and the biggest change seen on any social issue, including divorce, extramarital affairs and other issues.
Chambers disavowed reparative therapy at the annual Gay Christian Network conference in January 2012. “Alan has been moving this way for awhile … but this apology is much more explicit and leaves no room for support for change therapies or demonizing gays.” said Warren Throckmorton, a psychology professor at Grove City College who has long observed the ex-gay movement.
“Exodus has been a lighting rod for Christian discussion about homosexuality over the years and with today’s events will probably continue to be for awhile.”
John Paulk, who was spotted at a gay bar in Washington D.C. in 2000 and left his role as chairman of Exodus, also recently apologized for the reparative therapy he once promoted.
Chambers announced the closure of Exodus at the ministry’s 38th annual conference in Irvine, Calif. Local affiliated Exodus ministries, which are autonomous, will continue, but not under the name or umbrella of Exodus.
Exodus began in 1976 by a gay man, Frank Worthen. “Perhaps nothing has brought Exodus into the mainstream of evangelicalism more than its embrace by James Dobson’s Focus on the Family,” wrote Christianity Today in 2007. The ministry has faced some challenges in recent years, including a split with Willow Creek Community Church outside Chicago and dissolved partnerships.
In his apology, Chambers acknowledged stories of people who went to Exodus for help only to experience more trauma.
“I have heard stories of shame, sexual misconduct, and false hope,” he said. “In every case that has been brought to my attention, there has been swift action resulting in the removal of these leaders and/or their organizations. But rarely was there an apology or a public acknowledgement by me.”
On Thursday, journalist Lisa Ling’s program “God & Gays,” which features Chambers among others, will air on The Oprah Network. “The organization needs to shut down. Shut down!” a man in the trailer tells Chambers.
Back in my dim, dark past I was picked up one night in the Midnight Shift by a very cute guy. Nothing odd about that…until he took me to the back of the bar and introduced me to his boyfriend. The intention was obvious, they were both good looking men…and I didn’t say no. The sex was great and both guys seemed quite at ease in the threesome situation, and I stayed the night. However, the next morning was a real eye-opener…over breakfast, things took a real turn to the dark side…and I was caught right in the middle of it…with no idea what to do. Graeme…the guy who had picked me up the last evening…was relentlessly verbally abused by his partner, Peter. It was as though I wasn’t even there, as the abuse went on around me, and needless to say, it was a very uncomfortable breakfast. It seemed that Graeme could neither do, nor say, anything right. I never witnessed any physical abuse, but you could feel it underlying the verbals. Peter ordered Graeme to drive me home, and said he’d be timing it. I felt so bad for Graeme, as he was a really lovely, gentle guy. We got to my apartment building and I asked him if he would like to come in for a coffee…but he stated the obvious! If he wasn’t home in the allotted time, he’d cop it. A number of months later, I ran into Graeme in my local watering hole. The whole puck-up thing happened, though this time he was on his own. When I questioned what was happening with Peter, he said they’d parted company. I mentally breathed a sigh of relief. Graeme and I then went on to have a fuck-buddy thing for about 4 years. Last time I saw him…about 20 years ago now…he was in a happy relationship with another guy. I all my years on the gay scene, both amongst a large, close social circle, and in my day-zoo-day picks ups, fuck buddies and one night stands, that was the only incidence of gay domestic violence that I’ve ever encountered. However, it made me very aware of its existence, and how it can be so easily covered up just by presenting the normal semblance of a relationship. It did make me wonder just how much could have been going on amongst those I did know.
Domestic violence has become a “silent epidemic” in the gay and lesbian community despite being the subject of increasing scrutiny in heterosexual relationships, according to the AIDS Council of NSW.
Roughly one in three lesbian, gay bisexual, transgender, and intersex (LGBTI) couples experience domestic violence. Those statistics are echoed among the general population.
After years of fighting to prove their love is valid, LGBTI victims of domestic violence can feel like they are in another closet, making it harder to get help.
Russ Vickery was six months into his first gay relationship when the violence began.
“We went out for dinner and then drinks at a local pub … he got angry about something and the night ended with me having a broken nose,” Vickery says
Same-sex couple Russ Vickery (L) and Matthew Parsons have both been in domestic violence situations in their previous relationships. CREDIT: PAUL JEFFERS
“After the first time he was very apologetic and it was never going to happen again.” But it did happen, again and again over a period of five years, culminating in Vickery being thrown down a set of stairs at home in front of his children.
For Matthew Parsons, domestic violence came in other forms – psychological, financial and emotional abuse.
The smallest of triggers would set off a torrent of abuse, like the time he left the do not disturb sign on a hotel room door.
“When we returned, the room hadn’t been serviced for towels and so he flipped out and threw champagne, strawberries and chocolate across the room. I spent the night crying in the parking lot.”
Parsons had no control over his own finances either. The final straw came when his partner knowingly withheld from him the few dollars he needed to purchase lunch.
“I thought, you don’t even think of me as human, I’m just your play thing. That was a really horrible realisation to come to.”
It took both men years to realise they were experiencing domestic abuse, which is little talked about in the LGBTI community.
“He kept telling me that when two men get involved in a relationship, things turn physical,” says Vickery, who had been in a 17-year marriage prior to coming out. “I had no barometer so I just assumed that was how it worked.”
Parsons says the gay and lesbian community has spent so long trying to prove their love is valid, they are afraid to ruin it by admitting domestic abuse occurs.
“There’s an unspoken fear that if we start to tell the mainstream community that actually sometimes our relationships are toxic and horrible and abusive, then that will be used against us to say, ‘see it’s all unnatural and a sin anyway’.”
Vickery likens it to coming out a second time.
“A lot of people ask me why I didn’t leave [sooner] … but I’d come out and told everyone it was a wonderful thing. I didn’t want to come out again…”
ACON chief executive, Nicolas Parkhill, says for this reason, domestic violence is under-reported within the LGBTI community.
And because same-sex domestic violence “doesn’t look the same” as in heterosexual relationships, people don’t always recognise it, Parkhill says.
Unique to LGBTI victims is the fear the abusive partner will “out” them to family, friends and work colleagues, or reveal their HIV status.
Within the LGBTI community abuse is more frequently reported by women and transgender males than by gay men but Parkhill says more research is needed to determine the full extent of the problem.
He applauds the naming of Rosie Batty as Australian of the Year which has already raised the profile of domestic violence in the community, but says “the silent epidemic within this public profile raising is how that plays out in relationships that aren’t perceived as ‘the normal’.”
More needs to be done to raise awareness of domestic violence in gay and lesbian relationships, Parkhill says, and more government funding is needed for LGBTI-specific support services.
Matthew Parsons remembers calling a domestic violence hotline only to discover it was run by a Christian organisation.
“They were very unhelpful to say the least and I thought from that experience there wasn’t help out there, which isn’t true,” he says.
He eventually found help through the website Another Closet and counselling which encouraged him to do a “pack and dash” – fleeing while his partner was out.
The stair incident was the catalyst for Vickery to leave, but it still took him a year to come to terms with the relationship loss.
The men have been together now for four years and finally know what it is like to feel happy and safe.
Drawing on those experiences, they co-created a highly acclaimed cabaret show My Other Closet about domestic violence in gay relationships, for the Sydney Mardi Gras festival in 2013 and have plans to revive the show in Melbourne.
“[Our] horrible relationships … taught us both everything we never want to have in a relationship again,” Parsons says.
“We want to turn our negative experiences into a positive and put the message out there … that abuse is abuse and it’s the same in any relationship.”
The challenge of writing about 37 years of living with HIV/AIDS isn’t so much to write tomes about what actually was witnessed over that period. That is easy to do, and I could ramble on forever about it. The challenge lies in being objective and succinct, to tone down the schmaltz and sentimentality and cut to the chase. Not as easy as one may think, as these were the most challenging, relentlessly ruthless and heartbreaking years of my life. But if survival is the gauge of ones strength and tenacity, then I have come out at this end of it with flying colours. Indeed, the cup is half full!
The author at 65
So what was it really like in 1982 to be reading snippets in our local gay press about this mysterious illness in The States that seemed to be targeting gay men who frequented the saunas, and quickly killing them? Well, cynicism and disbelief to start with, and the surety that within a short period of time they would find an antibiotic to clear up yet another STD. Soon the snippets were to become columns, then pages as the mysterious and deadly illness leapt from the shores of America and found its way here.
Our response was mixed. The first recorded case of HIV at home was 1982, and the first death in 1983. We had our usual ratbags who yelled and screamed about God’s vengeance on the evil, sick and perverted gay lifestyle (obviously a different God to the compassionate, all-forgiving one that I had heard about), the advocates of hate who demanded quarantine for all infected persons, and those who either quietly or vocally wished that we would all die or just go away. Not that easy folks!
Thankfully, common sense prevailed and both the government and the grassroots gay community combined to put both AIDS Councils and NGO programs in place. Our quick response was instrumental in Australia always being at the forefront of HIV/AIDS care. Within 2 years every state had an AIDS Council under the national umbrella of NAPWA (National Association of People with AIDS), and the formation of support organisations such as The Bobby Goldsmith Foundation (named after the first person to die from AIDS in Australia), Community Support Network (CSN) and Ankali. Without these organisations life would have been grim for those infected. In 1985 testing was introduced. It was a bit of a strange affair in the early days. Due to hysteria and discrimination no one wanted their personal details on a database, so you chose a name, and Albion Street Centre issued you with a number that then became your ID. You had a blood test, and waited for two weeks – talk about high anxiety – to get your result. I had a mystery illness in 1982, a flu-type illness that wasn’t the flu, and already suspected that I had sero-converted and was going to come up HIV+. I was right. Counseling? Oh yeah, we had a lot of that back then. “You’ve got about 2 years to live”. Shrug shoulders “Okay”. And off we went knowing the inevitable was rapidly approaching, and it was time to PARTY!!! What else could you do?
However there were horror stories. The disgusting treatment of young Eve Van Grafhorst is something for all Australians to be ashamed of. Born in 1982, she was infected with HIV via a blood transfusion. When she attempted to enrol in her Kincumber pre-school in 1985, parents threatened to withdraw their children due to the (supposed) risk of infection. The family was literally hunted out of town, and forced to leave the country and go to NZ. I will never forget the sight of this poor, frail girl on her way to the airport. I, like many others, was horrified that this could happen in Australia. Thankfully, her NZ experience was quite the opposite, and she lived a relatively normal life until her death in 1993 at 11 years of age. Her parents received a letter from Lady Di praising her courage.
Eve van Grafhorst was diagnosed with HIV and hounded out of Australia, but her legacy endures
Meanwhile, the Australian nightmare was well and truly hitting home. My first close friend, Andrew Todd, died in 1986. At that time there was no dedicated AIDS ward, and Andrew was shifted between wards as beds were needed for other cases. He died on Boxing Day in A&E (called St Christopher’s ward, due to people usually just “travelling” through it on their way to a dedicated ward) at St, Vincent’s Hospital In Darlinghurst. It is interesting to note here that the Sisters of Charity, who founded this hospital, put the hospital at the centre of HIV care very early in the epidemic, and also provided palliative dare through the attached a Sacred Heart Hospice. I had the sad duty of ringing all my friends at a party to tell them the sad news. Party pooper recognition acknowledged! Ward 17 at St Vincent’s eventually became the dedicated AIDS ward, and for the next 10 years was never empty. Other hospitals such as Westmead hit the headlines for all the wrong reasons; full contamination clothing for those working with HIV people, rooms not being cleaned, meals left outside doors. Even the poor old mosquito copped a hiding as a means of contamination, along with toothbrushes, glasses, cutlery and crockery. An advertising campaign featuring the Grim Reaper bowling down poor people created an apocalyptic vision of HIV that scared the life out of everyone. It was quickly withdrawn. In the interim, my 2 years became 4, which became 6 followed by 8. My life became a haze of alcohol and cigarettes, not shared alone.
In the 80’s I held a lot of parties with anywhere from 40- 60 friends attending. By 1996, if I had tried to hold a party I would have been lucky to have dug up 10 friends to attend. In the blink of an eye my social circle was effectively wiped off the face of the earth. Hospitals, hospices, funerals and wakes became the dreaded regular events. It was death on a relentless and unforgiving scale. The Quilt Project became the focus of our sorrow, and it’s regular unfoldings and name readings were tear-filled times of remembrance and reminiscence, along with the yearly Candlelight Rally. I attended until I became so empty that I could no longer bear it. I submitted my names but no longer attended. In the early 90’s four friends died close together – two from AIDS, one a heart attack and one cancer. This was a particularly heavy blow as two of these friends had been regular “gutter drag” partners, and that part of my life effectively ended. In a perverse way, it seemed strange that the Big A wasn’t the only thing stalking our lives.
Ready to do a quilt unfolding at the Government Pavilion, Sydney Showgrounds, around 1991. From left Peter McCarthy, Peter Gilmore, Bevan Lambert, Steve Thompson, Tim Alderman.
Despite its reputation for being human Ratsac (the Concorde Study in France named it such, after conducting an unethical trial; turns out they were correct!) I started taking AZT when my CD4 count started to take a dive. Hard work, long hours, heavy drinking, chain smoking, a shit diet and emotional turmoil didn’t help. Pub culture became lifestyle. Did several drug trials – D4T, which was sort of successful, though the same class of drug as AZT. Also p24 VLP (Very Light Protein) which proposed that stimulating the p24 antigen may help control HIV. Total waste of my time. It did nothing. We started alternating drugs – 6 months on AZT, 6 on D4T, 6 on DDI, 6 on DDC. Perversely it seemed to keep the wolf from the door. Dosage was huge. Everyone on it ended up with kidney problems and peripheral neuropathy. Prophylactics added to the drug burden. In the meantime there was no HIV dental service and our teeth rotted or fell out due to bouts of candida. I left work in 1993 after being seriously knocked around by viral pneumonia which should have killed me…but didn’t.
Like many, I went on every drug or alternative trial that came my way. There are those who have described us guinea pigs as brave, or “heroes”, but we certainly didn’t feel like that at the time, despite it being a very selfless act. The thinking at such a desperate time was that…well, if it works for me, the benefit will flow onto everyone else! But there were, in the early days at least, more failures than successes. D4T:FAILURE…caused anaemia; P24-VLP:FAILURE…was hoped it would boost the p24 antigen – it did nothing: Goat Serum:FAILURE…though I did get a very scary skin rash from it; Vitrasert Implants: FAILURE…though due more to HAART eradicating the scourge of CMV retinitis. Were intended to leach Ganciclovir into the eye over a 9 month period, thus eliminating the need to have it injected into the eye regularly. Two minor operations to insert them, with an initial estimate of a 4% chance of developing cataracts. Turned out to be a 100% chance, thus further operations to remove the cataracts. Fun, baby!
I was shuffled onto the pension, and given rent subsidised housing by DOH (Department of Housing). The subsidy seemed like a good idea at the time. After all, weren’t we all eventually going to be killed by the Big H, so no one would be on it for that long? Famous last words! My alcohol consumption and chain smoking increased, if that was possible! Was losing weight at an alarming rate, and naturally no one noticed because I took to wearing baggy clothes to disguise it. Nothing quite like being delusional. Moved from Darlinghurst to Bondi. Nothing like moving away from the scene to help your health…not! Collapsed in the street, and admitted to St Vincent’s not with PCP as suspected but a collapsed lung. Two weeks later and a change of female GP’s saw me back in the doctor’s rooms while she read my hospital discharge report. Had they tested me for CMV retinitis? No! Was I having trouble with my vision? Yes, but I do wear glasses. Guess what? We’re sending you for a little holiday at Prince Henry Hospital (now closed). I was a little bit sick. Chronic CMV retinitis, chronic candida, chronic anemia, had 10 CD4 cells and weighed 48 kgs. Mmm, prognosis was not good. Well, it had been a good life. I was certainly joining a band of party people. But no! Life hadn’t finished with me yet. Protease Inhibitors had come along at an auspicious time, and within a fortnight I had been stolen from the arms of death. Mind you, that fortnight had been no picnic. Ganciclovir injections into the eye, Deca-Durabolin injections to help put weight back on, blood transfusions, and enough finger prick blood readings to last me the rest of my life. And the problems had just started for this return-to-lifer. Not dying when you are supposed to really fucks up your head space.
So started the next round of therapies. Peer Support groups; counselors; Caleo (Greek word which means “To Stick”, a treatment management group who help you maintain the impetus to take the billion pills a day (I was taking over 360 pills a week – anti-retrovirals, prophylactics, and pills to control side effects – at one stage) we were taking); clinics; dental care (now up and running); volunteer work (to keep one sane). What started out as volunteer work at the then PLWHA (NSW) Inc (now Positive Life) turned into paid employment as a research assistant. I started writing for “Talkabout” magazine, joined the Positive Speakers Bureau, and learnt to use a computer. A couple of stints back in full-time employment made me realise that big changes needed to be made with my life. By this time my health was pretty well back together. A couple of nights out pushed home just how few people I knew, however did lead to meeting my current (now ex) partner. A brief encounter with Indinivir sludge in my kidneys (which involved having a stent inserted then removed) also made me aware that for HIV+ people the unexpected can happen at any time. Yet another change of doctor. Self-empowerment had become an important issue, and I wanted a say in my health management, as distinct from being dictated to. Big changes were about to happen.
In 2000 David and I did a big (and expensive) holiday to the Red Centre. It was an amazing experience. Before leaving Sydney I had applied to the University of Technology in Sydney to do my degree in writing. Shortly after arriving back home I was informed that I had been accepted. Ah, the advantages of mature age AND disability. So spent three years doing my Graduate Certificate in Writing, was office- bearer for the Special Needs Collective…in fact I WAS the Special Needs Collective, and discovered I hated having to deal with the moronic “radicals” who called themselves the Student Association and did nothing except rant and rave, and waste student money. I was glad to leave uni. Towards the end of 2004 I decided to get my chef’s credentials from East Sydney TAFE, and crammed a 12-month course into 6 months. As much as I hated uni, I really loved TAFE and found it more grassroots and honest. David and I started Alderman Catering, a top-end catering business though it only lasted about 2 years as I found it very exhausting. I then sort of returned to my retail roots by opening a web site called Alderman Providore to sell Australian made gourmet grocery items. The site proved successful, and within 4 years I was opening my second site, this time specialising in tea, coffee and chocolate products. I got involved in a trial using Goat’s Serum to treat HIV, but again another waste of time. I did manage to get a skin rash from it, and managed to score a $1,000 for participating. In late 2009 the GFC hit, and online shopping took a major hit. After a disastrous Christmas that left me severely out if pocket, I decided to sell the business and put it behind me.
More eye problems followed, this time involving my blind eye. Back to the regular rounds at the Sydney Eye Hospital, and an injection of Avastin (a cancer drug that reduces blood flow) into the blind eye to stop it creating new blood supplies to an eye that couldn’t see. By this time, the interior of the bad eye was collapsing, and it took on an unnatural colour. Before this I hadn’t looked blind. Now I did! Scary how anyone you talk to can pick an anomaly – and stare at it while talking.
The next step, which sort of brings us up to date (this was 2011), was a major move. Plans to move north had been on the agenda for 10 years – in 2011 it finally happened, though we did jump the border which wasn’t in the original plan. No sooner were we there than my retina detached (I had been warned to eventually expect this, due to the amount of CMV scar tissue in the eye) in my one seeing eye…or rather was pushed off by all the scar tissue present from my original CMV infection. An emergency operation to scrape down the scar tissue, and replace the retina and fluid (called a vitrectomy) has seen my sight degenerate even further and I am now the proud owner of a white cane curtesy of Guide Dogs Queensland. It has become obvious that our two Jack Russell’s are not, despite their best of intentions, good seeing-eye dogs. I can see, though very poorly. A lot of life is a blur these days.
However, I am not going to complain. I have always enjoyed a challenge, and this presents yet another one. I gave up smoking 23 years ago, and drink only lightly and socially these days. I adopted a healthy diet and exercise program 10 years ago when I started getting unattractively over-weight and inactive.I have turned my life around by adopting this course of action. In 2013 I attended Southbank Institute of Technology in Brisbane and obtained my Certificate III in Fitness. I hoped this would lead on to becoming a Personal Trainer for mature-age and disabled people both individually and in conjunction with my local gyms. I was almost 60 by the time I finished. Just in time for the next stage of my life.
In 2014 David and I called an end to our 16 year relationship. It had run its course, and with a 14-year age gap…I’m the older…we were both at different stages of our lives. It was amicable, and we are still friends. However, it was the start of a year from hell. A disastrous 60th birthday followed, them an attack of shingles that was the worst Royal Brisbane Hospital’s Infectious Diseases Unit had ever seen, leading to an infection in the blisters that landed me in hospital with blood poisoning, followed by two weeks with a portable drip through their Hospital In The Home initiative (Neuralgia and numbness from this are still a problem 5 years down the line). Then our first rescue dog, Ampy, died. I was also faced with some serious decisions. With the parting of our ways, I could no longer afford to live in the house we were in being on a pension, and of the options open to me, returning to Sydney to move in with an ex from the 80s was the only viable one. I also made a nerve-wracking decision to have my blind eye removed, and replaced with a prosthetic. After years of ongoing problems with it, was time it came to an end, and the operation occurred in early 2015 just prior to my other dog, Benji, and myself returning to Sydney.
I stayed in Sydney only for as long as I needed to be there. I hated it! A cold, over-populated, rude city. Within 12-months, we…I include my housemate, who also came with me…moved to the Central Coast, where life is quiet, and more civilised. Life goes on…I’ve lived long enough now to start seeing the truth finally being told about many aspects of HIV – the high toxicity and ongoing problems caused by AZT, exploitation by Big Pharma, misuse of funding, unresearched and often inaccurate advice on therapies and treatments, the rushing through of many treatments that proved detrimental to those who took them. It’s time to clear the air, and take the sentimentality out of an often rose-coloured glasses view of the epidemic.
37 years eh! OMG where have those years gone? Despite all the discrimination, stress, anxiety, illness, deaths, survivor guilt and despair, there have been moments of great introspection, illumination, strength and enlightenment. That over-used word “empowerment” springs to mind and that is perhaps the one word that sums all those years up. Victim? No way! Survivor? Not in my words! And I have never been one to wallow in self pity. You just need to grab life by the balls, and get on with it. I trust that is what I have done.
Living in a hetero-normative world often demands men to act according to strict societal rules on “masculinity.”
GETTY IMAGES
I remember when I first thought my body was not good enough to be desired by other men. This feeling of disappointment with myself and envy of other men happened when I started going to gay bars and clubs. I noticed that men with defined muscles and often perfectly groomed facial hair received all the attention.
What they did not display was anything that was even slightly feminine.
Many gay men feel the pressure to have the perfect muscular body, which can be for their own self-confidence and health, but it may also be an attempt to exude society’s notion of masculinity in order to be desirable to other men. And part of this perception is due to toxic masculinity.
The term became known after Terry Kupers, a renowned American psychiatrist, published an article in 2005 titled, “Toxic Masculinity as a Barrier to Mental Health Treatment in Prison.” Kupers wrote that toxic masculinity was a “constellation of socially regressive male traits that serve to foster domination, the devaluation of women, homophobia, and wanton violence.”
MRBIG_PHOTOGRAPHY VIA GETTY IMAGES Muscular men getting more muscular.
“It (toxic masculinity) is when these traits and ideologies that (men) ascribe to as historically belonging to men, are exaggerated in a kind of dangerous form,” said Adam Davies, a doctoral candidate in education, gender and sexuality studies at the University of Toronto. “Many gay men therefore believe that in order to act like the ‘manliest’ man possible, this often means shunning anything that can even slightly be interpreted as feminine.”
“For a lot of gay men, just by being gay, there is this sense of insecurity of being a failure because they’re not performing their masculinity in the way that they (feel like they) are expected to,” said Davies.
Miah Mills, a Toronto resident, said that while he was very fortunate to have a non-gendered upbringing at home, his peers at school bullied him.
“They would police the whole boys do this/boys don’t do that nonsense,” said the 36-year-old. “Eventually, you police yourself.”
He said it took him many years to feel comfortable around effeminate gay men.
GETTY IMAGES Crowd of people in Berlin, Germany participate in a parade celebrating the LGBTQ community on June 21, 2014.
“I always knew that I should support them and be proud of them, but my first response was always to cringe. In them I saw the parts of myself that I hated. The parts of me that others saw in me and bullied me for.”
Alex McKenzie, a sexologist based in Montreal, said that he has also seen this same feeling of failure when working with predominantly LGBTQ2S men.
“This is a health risk because there is a constant dissonance between what they are trying to achieve versus what they actually want, which slowly has an effect on one’s mental health … it erodes your well-being the more it goes on,” says McKenzie. “I see a lot of issues in regards to anxiety come up, as well as depression, when people find themselves living in situations not right for them.”
Video above is a trailer for “Men Don’t Whisper,” a comedic short film about a gay couple emasculated at a sales conference, which screened at Sundance and SXSW earlier in September.
According to McKenzie, these mental health effects are also caused by dating apps, such as Grindr and Tinder.
“Dating apps are a phenomenon that started out as something innovative and fun, but has changed the landscape of dating and how we not only treat each other, but also how we view ourselves as individuals, which directly links to our self-esteem,” says McKenzie.
My own experiences on apps such as Grindr and Tinder have shown me that fit and active men (all traits seen as masculine) are the most desired men. While I consider myself to be fairly active, my lack of muscles and toned figure have made me close the apps at times wondering why I should even bother if I’m not the “ideal man.” Davies said this form of masculinity has always been put on a pedestal.
“In the (early 20th century) when gay men had different labels for themselves based on their gender expression, the feminized gay man was called ‘the fairy’ and was always seen as … the lowest denominator of gay communities,” said Davies. The word “fairy” was also often used as a homophobic slur.
A historical trope during the 1970s and 1980s that many gay men looked up to and tried to emulate was that of the “Castro” clone. Named after the historically gay Castro district in San Francisco, this stereotype was a rugged, muscular man with a moustache who would have sex with many different men without any attachments. I still find myself, from time to time, aspiring to be like one of them because of how they were so lusted after.
GETTY IMAGES Individuals congregate in the Castro District for the annual Pride celebration on June 27, 2015.
Rusty Souleymanov, a doctoral candidate at the University of Toronto’s Faculty of Social Work, whose doctoral work focused on the health and well being of substance-using gay, bisexual, as well as two-spirit and queer men in Toronto, said the desire to be seen as more masculine can also influence behaviours and lifestyles sometimes practiced by gay men.
“There’s this ongoing view that the manliest of men have a lot of casual bareback sex (penetrative sex without a condom) and also engage in substance use while having sex, and it can lead to a lot of health risks,” said Souleymanov, who has conducted research about HIV education among gay and bisexual men who use drugs.
The health effects that Souleymanov describes include higher rates of mental health issues and eating disorders on top of higher HIV rates. A 2007 article titled, “Eating Disorders in Diverse Lesbian, Gay and Bisexual Population,” by Matthew Feldman and Ilan Meyer showed that gay and bisexual men are up to 10 times more likely to suffer from eating disorders than heterosexual men.
None of the above is to say that toxic masculinity is the sole reason why these issues exist, but it does play an important role. Davies said that gay, bisexual and queer men need to be more vulnerable with each other.
For a lot of gay men, just by being gay, there is this sense of insecurity of being a failure because they’re not performing their masculinity in the way that they (feel like they) are expected to.
Adam Davies, a doctoral candidate
“A lot of men think that it isn’t masculine enough to talk about our emotions, our struggles and things that make us appear weak, but we need to be more open with each other,” said Davies. “We need to practice being more vulnerable with each other and start working to take away this stigma to really come together as a community.”
I am more at ease with my sense of self and my own body these days. Of course, there is still some work I can do on myself (I mean, who doesn’t?) but at least now I know that when I see these standards for gay men, they’re not what I should necessarily be. I would be lying if I said that I never feel a little bad looking at my scrawny self in the mirror, but I do know that it does not take away from my sense of masculinity.

















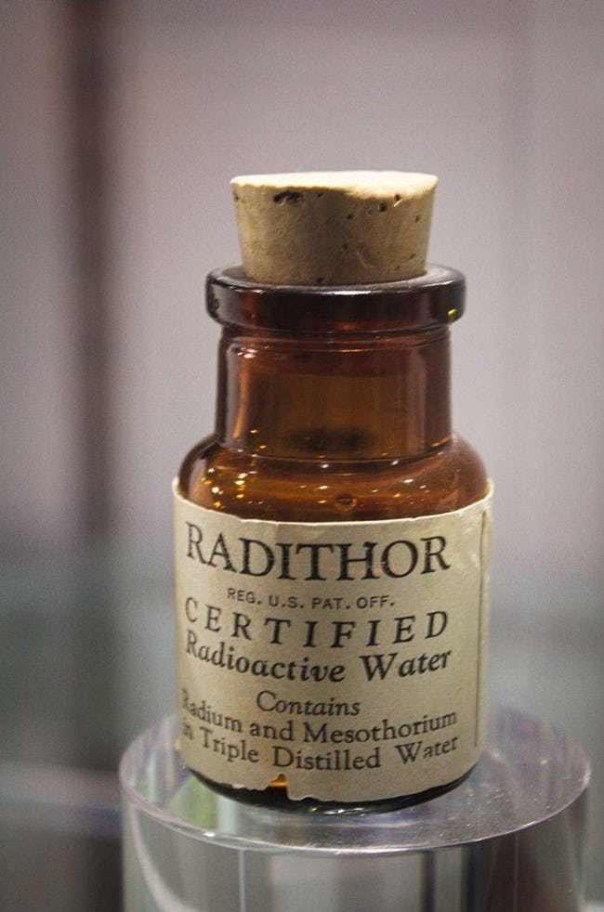



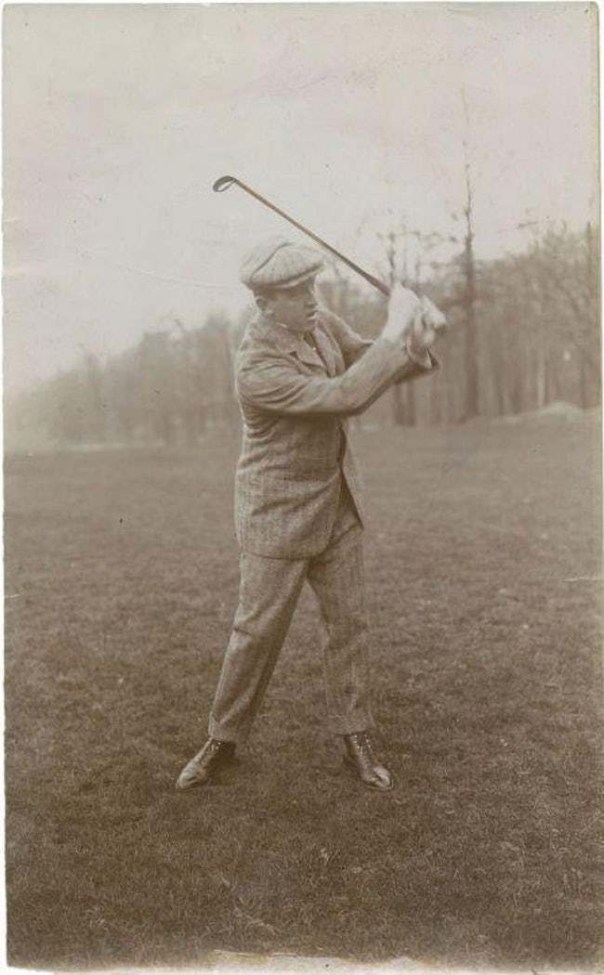

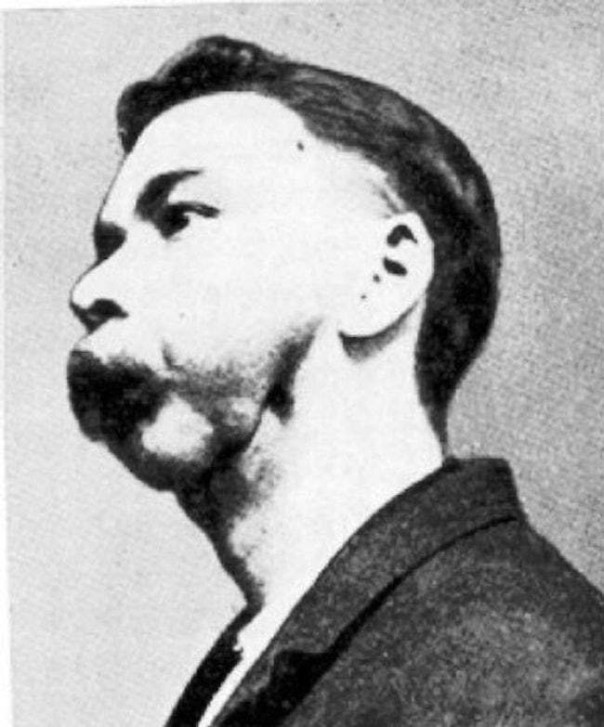

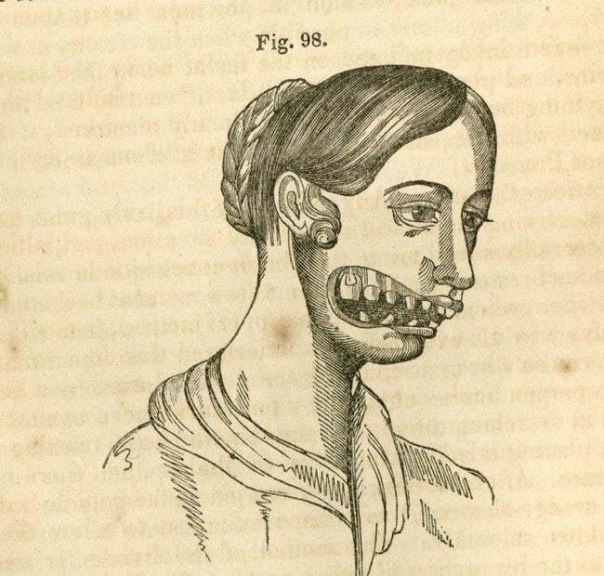






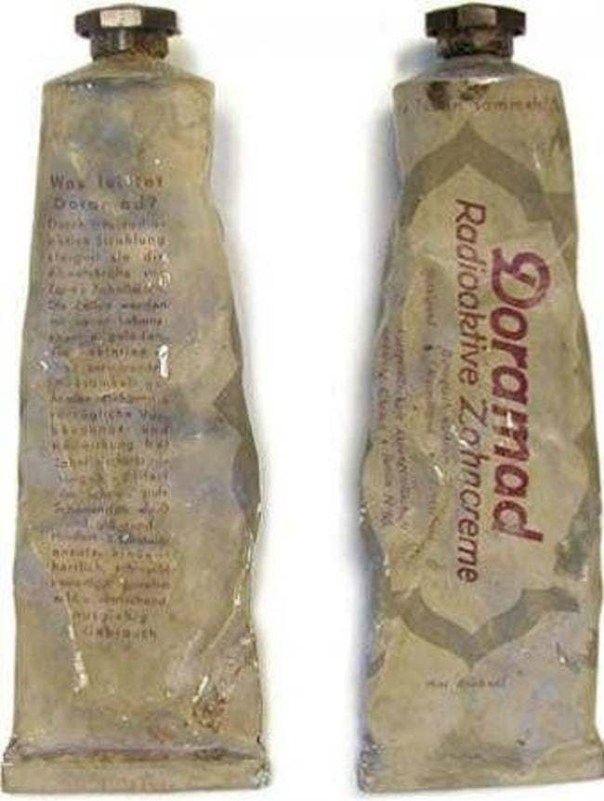


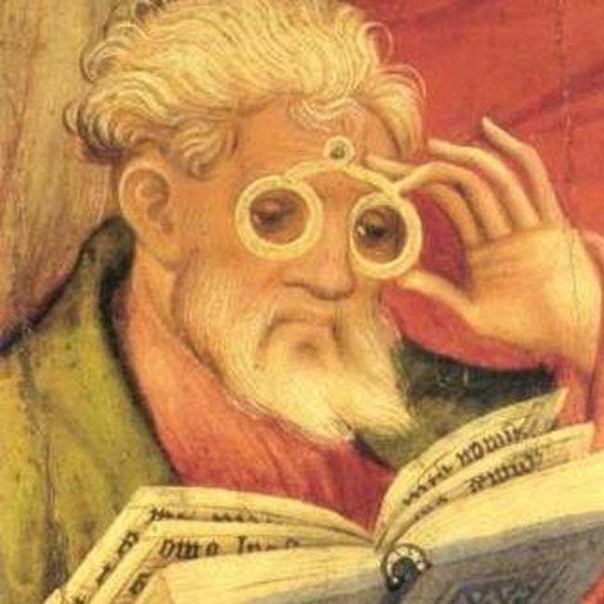
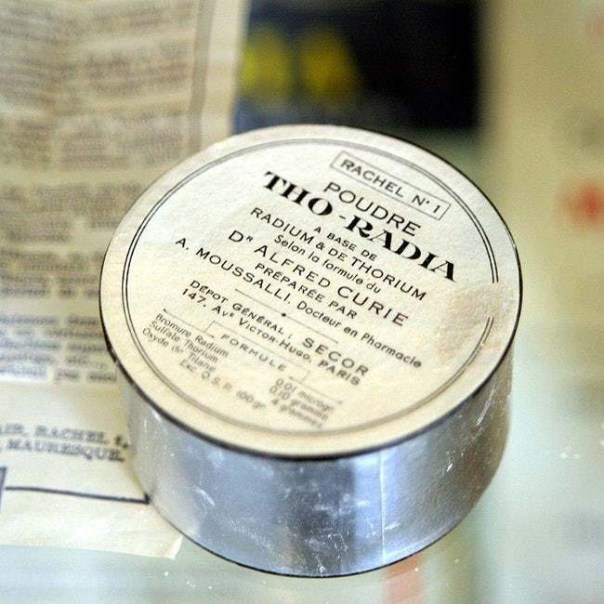

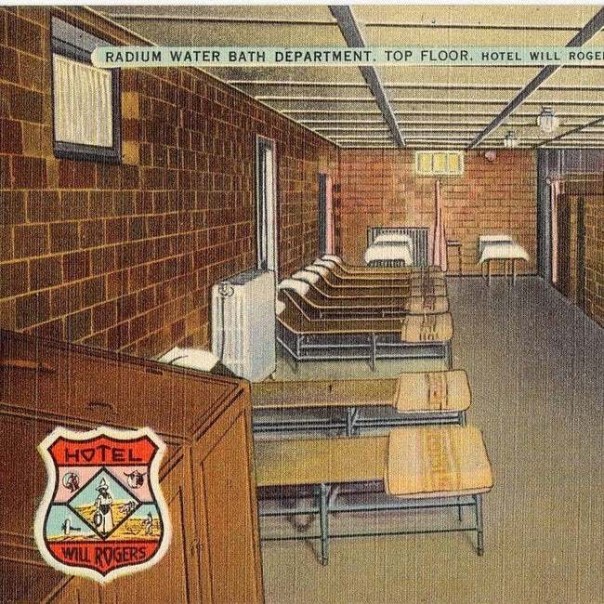


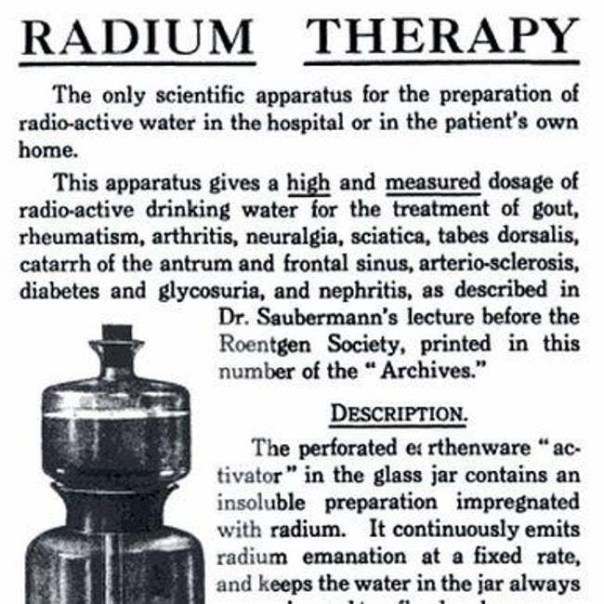




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.gif){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}