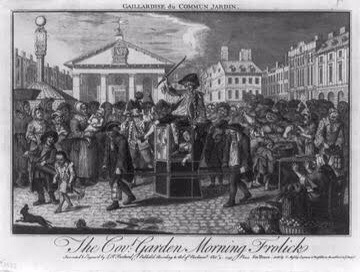
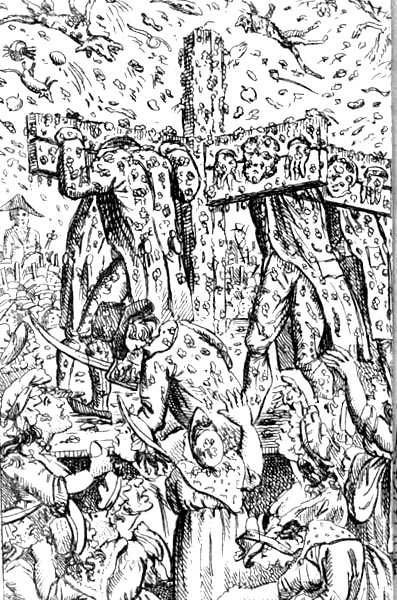
DescriptionExecution of Monks in Ghent because of Sodomy, 28 June 1578; Five monks accused of sodomy about to be burnt at the stake, left, and three others flogged, background centre, in Ghent town square. 1578 EtchingOn June 28, 1578, five Catholic monks were burnt to death in Ghent for homosexuality.
At our scene in the Spanish-controlled Low Countries, the revolt that would become known as the Eighty Years’ War and secure Dutch independence still had about 70 of those years to run.
Stadtholder William of Orange, aka William the Silent, has his hands full with the Habsburg forces determined to crush their disobedient subjects.
Half civil war, half proto-nationalist revolution, this conflict overlaid disputes over both political and religious authority, complicated by a catastrophic Spanish bankruptcy.
Of this compelling history much beyond our scope, the piece of most moment for our unfortunate monks was a grudging agreement to chill out the sectional suppression as part of a temporary truce between the warring sides. Said “slackening of persecution inspired Reformed public worship and attempts to topple the Catholic stewpot.” (Source)
Late in 1577, a political coup in the commercial powerhouse of Ghent did just that, part of a mini-Renaissance of Calvinist city-republics that Spanish arms would truncate in the 1580’s. But here in the 1570’s, the newly elevated slate of Calvinists implemented a “Reform” agenda that included aggressive moves against Catholic authority.
On 18-22 May [1578], the Reformed launched an attack on the four mendicant monasteries. Their churches were purified and made ready for Reformed worship. On 1 June the first public preaching was organized in the Dominican and Carmelite churches. (Source, a pdf)
Rumors of homosexuality in the religious orders swept the overheated city (assuming they were not put about intentionally), and this day opened a summer’s terror that saw 14 monks burned (pdf) for the love that dare not speak its name.
Kenneth Borris translates the inscription on the Franz Hogenberg image linked above thus:
“five monks are being burned in Flanders, in the city of Ghent. Four are Franciscans (Minnenbruder*) and the fifth Augustinian. Also three have been quickly flogged with switches on the market square as they deserve, because of their outrageous sexual offenses (unzuchtt) that greatly offended the authorities. That is why the four mendicant orders have now been driven out of Ghent.”
William the Silent, made of more statesmanlike stuff than these zealots, would actually enter Ghent himself the next year to disarm the ruling clique, realizing that firebrands were driving Catholic cities back into Spanish arms.
But he could not contain the schism. Spain ultimately kept the Catholic-leaning territories that today comprise Luxembourg and Belgium (including Ghent), while the Protestant Netherlands fought onward to independence.
* “Minnenbroder,” Borris explains, “may be a satiric pun on the word minne (which had come to mean debauchery), suggesting ‘brothers in lust’ as opposed to brotherly love. Hogenberg connects sodomy with ‘godlessness,’ as was common.”
The three men – ‘Ali bin Hittan bin Sa’id, Muhammad bin Suleyman bin Muhammad and Muhammad bin Khalil bin ‘Abdullah, all Saudi Arabian nationals, were publicly beheaded in Abha, Asir province, on 1 January 2002.
The Saudi Arabian Ministry of Interior issued a statement announcing that the three were convicted of homosexual acts, adding vaguely-worded charges of ‘luring Children’s rights and harming others’ without providing any further details. The trial proceedings – like most in Saudi Arabia – remain shrouded in secrecy.
Director of Amnesty International UK Kate Allen said:
‘The execution of these three men is yet another gesture of defiance of international standards by the Saudi Arabian government.
Widespread revulsion at these killings has led Amnesty International members to urgently contact the Saudi authorities expressing concern that these men may have been executed primarily because of their sexual orientation and seeking clarification of the exact charges and evidence brought against them.’
No detailed information regarding the trial proceedings for these individuals is yet known. Amnesty International is now also seeking urgent clarification of the names of any further prisoners under sentence of death due to their sexual orientation and calling for the commutation of their sentences.
This case is not an isolated case of people in Saudi Arabia being punished for alleged same-sex sexual relations. In April 2000 it was reported that a Saudi court had sentenced nine young men to prison sentences and up to 2,600 lashes each for ‘deviant sexual behaviour’. Six men were executed in July 2000 on charges partly relating to their sexual orientation and Amnesty International feared that these six may in fact have been among the nine men sentenced to the flogging and prison sentences. Like the recent executions, these six death penalties were carried out in Abha, Asir province.
This latest action by Amnesty International follows the publication last year of a report – Crimes of hate, conspiracy of silence – revealing that over 70 countries continue to criminalise same-sex relations, with some such ‘offences’ incurring the death penalty.
“Saudi Shame
Maryam Namazie
Published in Gay Times
June 2005
Gay people are routinely facing harassment, arrest, torture, flogging and execution in Saudi Arabia. It’s no wonder the gay rights group OutRage! has labelled Saudi Arabia one of the most homophobic countries in the world.
In May alone, as many as 92 men were arrested as ‘deviants’. On March 10, over 100 men were arrested after a raid for attending a gay wedding and found to be dancing and ‘behaving like women’. According to Amnesty International, 31 of the men were sentenced to imprisonment for 6 months to a year and up to 200 lashes each; four namely two Saudi Arabians, a Jordanian and a Yemeni were given two years’ imprisonment and 2,000 lashes. As is usual in Saudi Arabia, the sentences were passed in a closed session in which defence lawyers were barred. According to Human Rights Watch, the more than 70 men who had initially been released were subsequently summoned back and informed they had also been sentenced to one year’s imprisonment each.
These arrests closely follow the public beheading of Ahmed al-Enezi and Shahir al-Roubli, two gay lovers in Arar, in the north, for allegedly murdering a man who had found out about their relationship and was threatening to out them. The Saudi Interior Ministry’s statement announcing the execution said the two were found in a ‘shameful situation’, a term which is regularly used by the authorities to refer to homosexuality.
Whilst the reports are alarming, and seem to be escalating, one can be certain that these are only the tip of the iceberg. Most cases of persecution go unreported for the mere reason that the government is a dictatorship with strict censorship rules. For every report that reaches the international media and organisations, there are thousands of nameless, faceless individuals whose fate goes unreported. Under such circumstances, it is exceedingly difficult to collect facts and highlight the persecution gay people face. In the case of those arrested at the party for example, it was someone close to a defendant who alerted international organisations of the arrests and not official reports. The Saudi authorities seldom release information about arrests until after a trial and it is impossible to independently verify reports. All Saudi executions are also not systematically reported; officials continue to deny that the death penalty is applied for homosexuality ‘alone’. Of course there is evidence otherwise. On 1 January 2002, for example, Ali bin Hittan bin Sa’id, Muhammad bin Suleyman bin Muhammad and Muhammad bin Khalil bin ‘Abdullah were executed in Abha, Asir province, solely for their sexual orientation. And this is not a problem faced by gays in Saudi Arabia alone. In Iran, for example, on March 15, a government affiliated newspaper, Etemad, reported on the execution sentence of two men for homosexuality. No further reports have been received and their fate is unknown.
The abysmal situation of gay people in Saudi Arabia has to be looked at within the context of serious rights violations across the board. The beheadings of the two gay lovers in Arar brought the numbers beheaded for a variety of reasons this year alone to 24. People living in Saudi Arabia don’t have basic rights and freedoms and human rights violations are truly pervasive. Like all countries under Islamic rule, though, sexual ‘crimes’ are dealt with most severely because of their ‘shamefulness’ and ‘perversity’, especially since an Islamic state is usually most preoccupied with the control of sexuality and sex in order to assert its own ‘divine’ and ‘moral’ legitimacy.
Certainly, Islam is not unlike other religions when it comes to sex and sexuality. It is just as inherently homophobic and misogynist as other religions but there is one important fundamental difference and that is that it is a religion in power or vying for power in many countries in the 21st century. Homosexuality is condemned as ‘indecency’, ‘lewdness’, ‘degenerate’, ‘transgressing beyond bounds’ and in need of ‘punishment’ in the Koran. In the Hadith, which are the sayings of the prophet Mohammad and part of Sharia or Islamic laws, it clearly states: ‘Kill the one who sodomises and the one who lets it be done to him.’ Under Islamic Hudud laws, ‘illicit’ gay or straight sex are considered offences for which the punishment is mandatory and corporal in nature – including flogging, execution and stoning to death. These ancient religious texts become all the more relevant because they are translated into the laws of countries like Saudi Arabia and effect real live human beings. Whilst according to Amnesty International, more than 80 countries around the world criminalise same sex relations, eight punish it by death (Afghanistan, Iran, Mauritania, Nigeria – in states practising Sharia law, Pakistan, Saudi Arabia, the Sudan, and Yemen) – all of which one might add are countries or parts of countries under Islamic law.
This doesn’t mean that there isn’t an active gay community in Saudi Arabia, Iran or elsewhere or that gay tourists will be beheaded upon entry. Despite serious repercussions, people continue to live their lives, have sex and express their sexuality. Most Saudi cities have underground gay networks, which organise private parties. Some visitors find this pleasantly surprising and therefore mistakenly conclude that restrictions and repercussions are exaggerated. They are not. Or they often consider the legal restrictions and impositions as part of the ‘people’s culture and religion’ rather than that of the ruling class’. These visitors fail to make a distinction between the regime imposing these inhuman and medieval laws and the people forced to live under them.
Of course homophobia exists everywhere including in countries that do not impose Islamic law. But Islam in power or political Islam has raised homophobia to another dimension. Those of us who have fled political Islam know full well the levels of threats and intimidation those with ‘unchaste’ and ‘perverse’ lifestyles have faced and continue to face. The political Islam behind the arrests, floggings, and beheadings in Saudi Arabia is part of the same right wing reactionary movement, which hung sweet 16 year old Atefeh Rajabi from a city square in Iran for ‘acts incompatible with chastity’, beheaded prostitutes in Iraq and recently stoned to death a 29 year old woman, Amina, accused by her husband of adultery, in Afghanistan. [As I mentioned, in many cases, we are left with only a first name or no name at all.]
This movement is also permeating into life in Britain and the west as well. Demands for child veiling, Islamic schools and a Sharia court in Britain for Muslims as well as Ken Livingstone’s love affair with al-Qaradawi are all evidence of this fact. In Saudi Arabia and Iran, political Islam kills, maims and brutalises, but here the ‘moderate Islamic scholar’ Qaradawi’s support for women’s ‘modesty’ and his condemnation of sexual acts as ‘perversions’ are deemed mere abstract questions of freedom of speech or academic/theological debates. Don’t be fooled. They are all part and parcel of the same movement and implement Islamic rules as soon as they have any power. [By the way, it was also an ‘Islamic scholar’ who issued the sentence for Amina’s stoning to death in Afghanistan.]
The rise of political Islam here in Britain is affecting countless women, gays, and others who have sought refuge and safety in Britain from it. Moreover, whilst the UK government has close relations with countries like Saudi Arabia and Iran, it continues to refuse and deport its victims. Just last year, Hussein Nasseri, 26, a gay man who feared he would be executed if he were deported to Iran killed himself after the Home Office turned down his second appeal for asylum.
To make matters worse, any attempt to criticise Islamic laws and states are now being deemed racist and Islamophobic. Even the Saudi government itself has labelled criticism of its policies and practices as such. Clearly though, the targets of racism and discrimination are human beings not beliefs or ideas belonging to or attributed to them nor social or political movements associated with belief systems. Such labels are often used by Islamic states and their apologists in the west to silence any criticism and opposition.
Nonetheless, the Saudi government and its likes need to know that the world is watching them when they abuse rights with such impunity. They cannot be allowed to torture, imprison and behead gay people and others under cover of secrecy and carry on with business as usual with western governments such as the UK government, which has military links with the kingdom. Most importantly, though, those being abused and violated need to know they are not alone. That they are not just nameless, faceless individuals languishing in prison or facing torture and execution. They need to know that there are other people all over the world who will not stand by and remain silent.”
References
Nine men and one notorious women died at Tyburn on this date in 1726 at a more than usually raucous execution-day.“At the Place of Execution, Map got himself loose, threw himself out of the Halter, and jump’d 3 or 4 Yards from the Cart, upon the Heads of the numerous Crowd of People, but the Officers following after him, wounded him with their Pikes, and the Executioner and some others soon brought him back again,” the Ordinary’s account remarked. “Vigous got himself free of the Halter also, which was immediately observ’d: Gillingham was the more desirous of Prayers, having the Night before taken Poyson, and conscious of his Guilt.”
And that’s just what was happening under the nooses.
Out in the audience,
Just before the Execution, a Scaffold that had been built near Tyburn, and had about 150 People upon it, fell down. A Snuff Box Maker in Castle-Street, and a Gentleman then not known, were, as ’tis believed, mortally Wounded; and about 12 other Men and Women, Maimed and Wounded in a most cruel Manner: Some having their Legs, others their Arms, &c. broke.
Some part of the Scaffold being left standing, the Mob gathered upon it again in Numbers; and in about Half an Hour more, that also fell down, and several were hurt. Soon after another Scaffold broke down, with about 100 Persons upon it; but the People that were damaged by it, being immediately carried off on Mens Backs, and in Coaches, we must defer the Particulars of that Mischief … (Daily Journal, May 10, 1726)
We will leave for a future May 9th the notorious fate of the woman, Catherine Hayes, and focus for this post on the fate of the notorious men: sodomites Gabriel Lawrence, William Griffin, and Thomas Wright.
A mere three months before, this trio had been among dozens of men rounded up in a raid on London’s thriving “molly house”.
These establishments catered to what we might anachronistically call the gay scene of Georgian London — or the molly scene, if you like, from the slang term for effeminate, cross-dressing, or homosexual men encompassing a panoply of alternate sexual identities and preferences. What these behaviors “among Christians not to be named” had in common, of course, was the opprobrium of the surrounding world.
Rictor Norton, who keeps the voluminous Homosexuality in Eighteenth-Century Enland site and wrote a book about Mother Clap’s Molly House, records a 1726 letter to the editor demanding an exemplary punishment to check the misuse of genitalia.
It being too notorious, that there are vile Clubs of Miscreants in and about this City, who meet to Practise and Propagate the detestable Sin of Sodomy, a Crime which drew down the flaming Vengeance of God upon the City of Sodom, in a Day when they had not that Light which we are bless’d with now, ’tis humbly propos’d that the following Method may not only destroy the Practice, but blot out the Names of the monstrous Wretches from under Heaven, viz. when any are Detected, Prosecuted and Convicted, that after Sentence Pronounc’d, the Common Hangman tie him Hand and Foot before the Judge’s Face in open Court, that a Skilful Surgeon be provided immediately to take out his Testicles, and that then the Hangman sear up his Scrotum with an hot Iron, as in Cases of burning in the Hand.
Old Blighty was never favored with courtroom scrotum-searings, but connoisseurs of same-sex love “must risque our necks for” it well into the next century.
But what pleasures welcomed the man who was ready to wager his life! An informant reported from that same Mother Clap’s that he
found between 40 and 50 Men making Love to one another, as they call’d it. Sometimes they would sit on one another’s Laps, kissing in a lewd Manner, and using their Hands indecently. Then they would get up, Dance and make Curtsies, and mimick the voices of Women. O, Fie, Sir! – Pray, Sir. – Dear Sir. Lord, how can you serve me so? – I swear I’ll cry out. – You’re a wicked Devil. – And you’re a bold Face. – Eh ye little dear Toad! Come, buss! – Then they’d hug, and play, and toy, and go out by Couples into another Room on the same Floor, to be marry’d, as they call’d it.
Several such informers were stalking the city’s molly-houses in the 1720s, goaded (or forced) by both police and private bluenoses. One of the resulting court records notes that “[t]he discovering of the Molly Houses, was chiefly owing to a Quarrel betwixt Mark Partridge and – Harrington: For upon this Quarrel Partridge to be revenged on Harrington, had blab’d something of the Secret, and afterwards gave a large Information of a great many others.”
Many lives hung on this lover’s spat. Mother Clap’s was raided in February 1726, but it was just the most famous of a whole series that forced into public awareness “a new, distinct molly ‘sodomite’ identity.”
The saving grace for the twoscore arrestees at Mother Clap’s was that even in Bloody Code England, a fairly high bar was required to execute for same-sex sodomy: “penetratio, that is res in re“ (“thing in thing”)* — often quite difficult to prove.** As nobody had actually been caught in flagrante delicto, most of those initially arrested were simply released un-charged.
But the informants raise their scaly heads once more here: as they were themselves habitues of the molly circuit, they could provide firsthand eyewitness testimony about the acts of buggery several men had committed with them.
Five men were put on trial for their lives in April on the strength of accusations made by informants Mark Partridge, Thomas Newton, and Edward Courtney. The cases are described in some detail at Norton’s site: Gabriel Lawrence and William Griffin, both 43-year-old married men, were Mother Clap regulars who implausibly claimed to have no idea it was a molly house. (The place was a coffee shop/tavern.) Griffin actually lived there. Both these men were easily condemned but refused to the end to admit their proclivities to the Newgate Ordinary, and insisted that they had been framed.
Thomas Wright, seller of ale, had gone so far to set up his own molly house where he both slept with Newton, and procured Newton for his other customers. Wright, who “inclin’d to the Anabaptist-Way,” also said that Newton had perjured himself; nevertheless, he “could not deny his following this abominable Courses, only he refus’d to make particular Confessions.”
A third informant keyed two additional capital trials that didn’t end at Tyburn. George Kedger (Keger) and George Whittle (Whytle) both mounted much stronger defenses casting much greater doubt on the circumstances of their entrapment.
Charged with taking Courtney into his bed, Kedger contended that he had in fact resisted Courtney’s advances until the latter threatened to “swear my Life away”. Kedger was condemned, but pardoned. Whittle did still better by forcing his accuser to admit that he was a convict three times over and insinuating that rumors about his buggery were started by a disgruntled lodger. With a parade of character witnesses at his back, Whittle was acquitted outright.
* This was also the standard for same-sex rape; we’ve seen in these pages a man’s life hang on a question of just the tip.
** Attempted buggery — a charge which could result from making a sexual advance on another man that he rejected, or as a judicial punt when same-sex activity was afoot but no penetration could be proven — might land one a fine and a trip to the pillory. This was no mean sentence; the pillory could be quite a dangerous (sometimes lethal) ordeal for homosexuals or for anyone else.
Mother Clap herself, whose molly house we have referred to throughout this post, was also pilloried, not executed. Her eventual fate is not known; a marker in Holborn notes the former site of her famous establishment.
Gabriel Lawrence’s Old Bailey Sodomy Trial 20th April 1726
Gabriel Lawrence , was indicted for feloniously committing with Thomas Newton , aged 30 Years, the heinous and detestable Sin of Sodomy . Thomas Newton thus depos’d. At the End of last June, one Peter Bavidge (who is not yet taken) and – Eccleston (who dy’d last Week in Newgate) carry’d me to the House of Margaret Clap (who is now in the Compter) and there I first became acquainted with the Prisoner. Mrs. Clap’s House was next to the Bunch of Grapes in Field-lane, Holbourn . It bore the publick Character of a Place of Entertainment for Sodomites, and for the better Conveniency of her Customers, she had provided Beds in every Room in her House. She usually had 30 or 40 of such Persons there every Night, but more especially on a Sunday. I was conducted up one pair of Stairs, and by the Perswasions of Bavidge (who was present all the Time) I suffer’d the Prisoner to commit the said Crime. He has attempted the same since that Time, but I never would permit him any more. When Mrs. Clap was taken up, in February last, I went to put in Bail for her; at which Time, Mr. Williams, and Mr. Willis told me, they believ’d I could give Information, which I promis’d to do, and I went next Day, and gave Information accordingly. – Samuel Stephens thus depos’d. Mrs. Clap’s House was notorious for being a Molly-House. – In order to detect some that frequented it, I have been there several Times, and seen 20 or 30 of ’em together, making Love, as they call’d it, in a very indecent Manner. Then they used to go out by Pairs, into another Room, and at their return, they would tell what they had been doing together, which they call’d marrying. The Prisoner acknowledg’d, that he had been several Times at Clap’s House, but never knew that it was a Rendesvouz for such Persons. – He call’d several to his Character. Henry Hoxan thus depos’d. I have kept the Prisoner Company, and served him with Milk these 18 Years, for he is a Milk Man , and I am a Cow-Keeper, I have been with him at the Oxfordshire Feast, and there we have both got drink, and come Home together in a Coach, and yet he never offer’d any such thing to me. Thomas Fuller thus depos’d. The Prisoner married my Daughter, 18 Years ago; She has been dead these 7 Years, and he has a Girl by her, that is 13 Years old. – Several others deposd, that he was a very sober Man, and that they had often been in his Company when he was drunk; but never found him inclinable to such Practices. Guilty . Death . He was a 2d. Time indicted, for committing Sodomy with Mark Partridge , Nov. 10 . But being Convicted of the Former, he was not Try’d for this.
“The Ordinary’s Account of Gabriel Lawrence.
Gabriel Lawrence, aged 43 Years, was a Papist, and did not make any particular Confessions to me. He kept the Chapel with the rest for the most part; was always very grave,, and made frequent Responces with the rest, and said the Lord’s Prayer and Creed after me. He owned himself of the Romish Communion; but said, that he had a great Liking to the Church of England, and could communicate with them; but this I would not allow, unless he renounced his Error. He said Newton had perjured himself, and that in all his Life he had never been guilty of that detestable Sin; but that he had liv’d many Years with a Wife who had born several Children, and kept a good sober House. ——
At the Place of Execution he said, that a certain Person had injured him when he took him before a Justice of the Peace, who committed him, in swearing or affirming, that fifteen Years ago he had been taken up for that unnatural Sin, and that it cost him Twenty Pounds, to get himself free, which, he said, was utterly false; for, ’till this Time, he was never suspected.
He was hanged at Tyburn, on Monday, May 9, 1726.”
William Griffin’s Old Bailey Sodomy Trial 20th April 1726
William Griffin , was indicted for Committing Sodomy with Thomas Newton , May 10 . Thomas Newton thus depos’d. The Prisoner and Thomas Phillips , (who is since absconded,) were Lodgers for near 2 Years at Clap’s House. I went up stairs, while the Prisoner was a Bed, and there he committed the Act with me. Samuel Stevens depos’d, That he had seen the Prisoner, and his Gang at Clap’s House. Guilty . Death .
“The Ordinary’s Account of William Griffin.
William Griffin, aged forty-three Years, an Upholsterer by Trade, in Southwark; had, as he said, been a Man of good Business, but, haveing squandered away, or lost his Money, was fallen into Poverty. He denied the Fact for which he died, calling Newton, the Evidence, perjured; and saying, that the abominable Sin was always the Aversion of his Soul; for he had lived many Years with a good virtuous Wife, who had several Children, two of which, a Boy and a Girl, are living; and, he said, both of them behave mighty well, and to the Satisfaction of all concerned with them: And he hop’d that the World would not be so unjust, as to upbraid his poor Children with his unfortunate Death.
At the Place of Execution, —— Griffin would not own the Commission of that detestable Sin.
He was hanged at Tyburn, on Monday, May 9, 1726.”
Thomas Wright’s Old Bailey Sodomite Trial 20th April 1726
Thomas Wright , was indicted for committing Buggery with Thomas Newton . Jan 10 1724- 5. Thomas Newton thus depos’d. Last January 12 Month, the Prisoner had the Carnal Use of my Body at his own House, in Christophers Alley in Moor-fields : He was a Wooll-Comber by Trade, but he sold a Dram among such Company as came to his House. – He afterwards remov’d to Beech Lane, and there kept Rooms for the entertainment of Sodomites. He sold Ale, but he had it from other Ale-houses: He has often fetch’d me to oblige Company in that way, and especially to one Gregory Turner . William Davison and – Sellars thus depos’d. The discovering of the Molly Houses, was chiefly owing to a Quarrel betwixt Mark Partridge and – Harrington: For upon this Quarrel Partridge to be revenged on Herrington, had blab’d something of the Secret, and afterwards gave a large Information of a great many others. The Mollies had heard something of the first Discovery, but did not imagine how far he had proceeded, and what further Designs he had upon them. – By his means we were introduced to the Company, at the Prisoners Lodging’s. There were 8 or 9 of them in a large Room, one was playing upon a Fiddle, and others were one while dancing in obscene Postures, and other while Singing baudy Songs, and talking leudly, and Acting a great many Indecencies. – But they look’d a skew upon Mark Partridge , and call’d him a treacherous, blowing-up Mollying Bitch, and threatned that they’d Massacre any body that betray’d them . The Prisoner was very fond of us, and kist us all at parting in a most indecent manner, Edward Sanders in behalf of the Prisoner depos’d, That he never heard any such report of the Prisoner before; That he was born and bred at Newbury, and was esteem’d an honest Man, The Jury found him Guilty . Death .
May 9 – 1726 – Three Men are Publicly Hanged for Sodomy at Tyburn
The Productive Leisure Network
Gabriel Lawrence, William Griffin, and Thomas Wright were initially arrested after a raid by authorities at a “molly house” owned by a Margaret Clap. Molly houses were gathering places for homosexual men in eighteenth century England. Since the reign of Henry VIII, homosexual sex between men, better known as “buggery” or “sodomy,” was illegal. On the other hand, its prosecution was varied, and in the early eighteenth century, after the Glorious Revolution and the Hanoverian Succession, the desire to prosecute men on sodomy charges was increased through the Society for the Reformation of Manners. The problem was the actual way to prosecute sodomy, which led to a reliance on informants, who were usually hustlers and male prostitutes who were arrested on other charges. That is how Margaret Clap’s establishment was raided and how evidence was brought against Lawrence, Griffin, and Wright. All three men tried to present some evidence that they had no idea that Clap’s house was a molly house, but the juries didn’t buy it. Thus, they were publicly hanged at Tyburn for the crime of sodomy, a public spectacle which was relatively rare in the history of Britain.
CITATION: If you refer to this Web page, please use the following citation:Rictor Norton (Ed.), “The Trial of Gabriel Lawrence, 1726”, Homosexuality in Eighteenth-Century England: A Sourcebook. 1 Dec. 1999, updated 20 June 2008 <http://www.rictornorton.co.uk/eighteen/1726lawr.htm>.
On June 17th in 1660, in the Netherlands’ little settlement on the tip of Manhattan Island, New Amsterdam, Jan Quisthout van der Linde was sentenced “to be taken to the place of execution and there stripped of his arms, his sword to be broken at his feet, and he to be then tied in a sack and cast into the river and drowned until dead.”We do not have an indication of the date this sentence was carried out, if it were not immediate.
It was an unusual execution for an unnatural crime: Quisthout had been found guilty of sodomizing his servant.
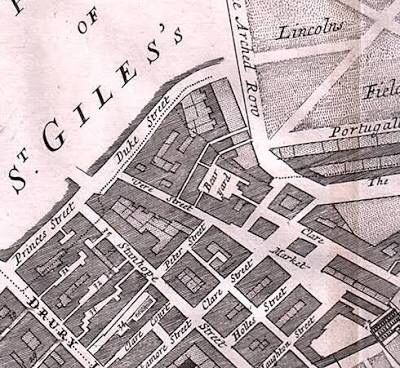
New Amsterdam is here just four years away from its seizure by the English, who rechristened it New York;* dour, peg-legged Calvinist Peter Stuyvesant had been hustling for 13 years to put the tenuous little settlement on some sort of sustainable, defensible footing even as its neighbor English colonies in Massachusetts, Connecticut, and Rhode Island grew to dwarf little Manhattan.
Stuyvesant was a crusty boss.** He’d been crestfallen on arrival to his new assignment to find New Amsterdam a rough-edged melting pot city with livestock roaming the streets, a slurry of languages (and religions), and dockside brawls spilling out of seedy taverns.†
The “Castello Plan” map from 1660 shows the germ of Manhattan’s present-day layout. The defensive wall spanning the island on the right gives us Wall Street.
His horror was practical as well as moral: the little colony, a few hundred souls when he took over and perhaps 1,500 when the English finally deposed him, was in danger on all sides and the cash-strapped West India Company was both slow and miserly in response to Stuyvesant’s desperate pleas for men and material. But the horror was also moral. Stuyvesant enforced a whole slew of unpopular injunctions against drunkenness, fisticuffs, and fouling public streets with refuse, and actually had to be reined in by the West India Company board when he got so overbearing as to try shouldering out Jews and prying into the devotional habits of suspected Quakers.
A paragon of rectitude like Stuyvesant was in no way about to turn a blind eye to casual Atlantic-world buggery.
Even his lax predecessor had come down hard on a previous sodomy case, viewing that sin as an existential threat to their depraved port: “such a man is not worthy to associate with mankind and the crime on account of its heinousness may not be tolerated or suffered, in order that the wrath of God may not descend upon us as it did upon Sodom.”
The crime that we might see here with modern eyes, rape, was in no way foremost to Stuyvesant et al. The boy, an Amsterdam orphan named Hendrick Harmensen, stayed out of the drowning-sack — but he was whipped for same-sex contact and ordered “sent to some other place by the first opportunity” even though that very sentence acknowledged that it was Quisthout who had “committed by force the above crime” on the lad.
The diary (pdf) of a man imprisoned at Newgate recorded for this date in 1819 that
A man was hanged this morning for an unnatural crime. Had my windows fastened up but could not sleep. They began putting up the scaffold at 4 o’clock. The tolling of the bell at 8 was frightful. I heard the crash of the drop falling and a woman screech violently at the same moment. Instantly afterwards, the sound of the pye man crying, “all hot, all hot.” ‘Tis dreadful hanging a man for this practice.* There are two, a man and boy now in jail, who were caught in flagrante delictu — and yet only sentenced to two years imprisonment. The poor wretch was half dead, so they told me, before he was hanged.
Of this poor soul fallen away into the indifferent cries of the pye-man we have this from The Morning Post of December 30, 1819.
John Markham was obscure, no doubt; his condemnation literally was for unspeakable acts, since it barely rates a line at all in the Old Bailey’s archives.
But the aural observer of his death was not obscure at all.
John Hobhouse, though he would eventually become the first Baron Broughton, was a buddy of the queer-friendly Lord Byron (the fourth canto of Byron’s Childe Harold’s Pilgrimage is dedicated to Hobhouse). Hobhouse was also a prominent radical rabble-rouser, which is precisely why he was in Newgate on the day of Markham’s hanging.
All of this occurred in the tense wake of the Peterloo Massacre, which saw British cavalry ride down their countrymen in Manchester for assembling to demand the reform of a parliament long grown egregiously unrepresentative. (Manchester was a case in point: it had no M.P. at all based on a centuries-old allocation of boroughs even though it had now boomed into one of the realm’s leading centers of industry.**)
Following the Peterloo outrage, our correspondent Mr. Hobhouse had suggested in one of his many combative pamphlets that absent such brutal exertions the members of Parliament “would be pulled out by their ears” at the hands of an aggrieved populace. Given the all-too-recent aftermath of the Napoleonic Wars — and their antecedent, the French Revolution — the potential threat in these words seemed to the powers that be a step beyond mere colorful rhetoric.
Accordingly, the House of Commons judged Hobhouse guilty of a breach of privilege and had him arrested earlier that same December. His cause more advanced by the martyrdom than inconvenienced by a gentleman’s loose detention — Hobhouse’s at-liberty associates not only held political meetings in his ample prison apartments but planned and advertised them in advance — the man won election to that selfsame House of Commons from Westminster the following March.
* A few days later, Hobhouse will record in his diary that he has been told that Markham “had committed his crime with a pauper in a workhouse on a coffin.”
** The U.K. finally enacted parliamentary reform in 1832. A few years after that, it even stopped hanging people for sodomy.
EXECUTION. — Yesterday morning, at an early hour, considerable numbers of spectators assembled before the Debtors’ door at Newgate, to witness the execution of William North, convicted in september Sessions of an unnatural crime.
The wretched culprit was 54 years of age, and had a wife living.
On his trial, he appeared a fine, stout, robust man, and strongly denied his guilt. On his being brought before the Sheriffs yesterday morning, he appeared to have grown at least ten years older, during the five months he has been in a condemned cell, with the horrid prospect before him of dying a violent death. His body had wasted to the mere anatomy of a man, his cheeks had sunk, his eyes had become hollow, and such was his weakness, that he could scarcely stand without support.
Though the consolations of religion were frequently offered to him, yet he could not sufficiently calm his mind to listen, or participate in them, even to the moment of his death. Sunday night he could not sleep, his mouth was parched with a burning fever; he occasionaqlly ejaculated “Oh God!” and “I’m lost;” and at other times he appeared quite childish; his imbecility of mind seemed to correspond with the weakness of his body. He exclaimed on one occasion “I have suffered sufficient punishment in this prison to atone for the crimes I have committed;” and when the Rev. Dr. Cotton and Mr. Baker, who attended him, asked him if he believed in Christ, and felt that he was a sinner? He replied “I pray, but cannot feel.”
The Sacrament of the Lord’s Supper was not administered to him, probably on account of his occasional delirium, and the generally disordered state of his mental faculties.
At five minutes before eight yesterday morning he was pinioned by the executioner in the press room, in the presence of the sheriffs and officers of the goal. As St. Sepulchre’s church clock struck eight, the culprit, carrying the rope, attended by the executioner, and clergyman, moved in procession with the sheriffs, &c. on to the scaffold.
On arriving at the third station, the prison bell tolled, and Dr. Cotton commenced at the same moment reading the funeral service “I am the resurrection and the life,” &c. of which the wretched man seemed to be totally regardless. On his being assisted up the steps of the scaffold, reason returned; he became aware of the dreadful death to which he was about to be consigned; his looks of terror were frightful; his expression of horror, when the rope was being placed round his neck, made every spectator shudder.
It was one of the most trying scenes to the clergymen they ever witnessed — never appeared a man so unprepared, so unresigned to his fate. — The signal being given the drop fell, and the criminal expired in less than a minute. He never struggled after he fell.
The body hung an hour, and was then cut down for interment. — The six unhappy men who are doomed to suffer on to-morrow morning, appear to be perfectly resigned to their fate.
News Paper Reports
Saturday 22 February 1823
His Majesty was pleased to order the following for execution: . . . Wm. North, convicted last September Sessions of an unnatural crime, on Monday morning next. (Morning Chronicle)
Tuesday, 25 February 1823
EXECUTION. – Yesterday morning, at an early hour, considerable numbers of spectators assembled before the Debtors’ door at Newgate, to witness the execution of William North, convicted in September Sessions of an unnatural crime. The wretched culprit was 54 years of age, and had a wife living. On his trial, he appeared a fine, stout, robust man, and strongly denied his guilt. On his being brought before the Sheriffs yesterday morning, he appeared to have grown at least ten years older, during the five months he has been in a condemned cell, with the horrid prospect before him of dying a violent death. His body had wasted to the mere anatomy of a man, his cheeks had sunk, his eyes had become hollow, and such was his weakness, that he could scarcely stand without support. Though the consolations of religion were frequently offered to him, yet he could not sufficiently calm his mind to listen, or participate in them, even to the moment of his death. Sunday night he could not sleep, his mouth was parched with a burning fever; he occasionaqlly ejaculated “Oh God!” and “I’m lost;” and at other times he appeared quite childish; his imbecility of mind seemed to correspond with the weakness of his body. He exclaimed on one occasion “I have suffered sufficient punishment in this prison to atone for the crimes I have committed;” and when the Rev. Dr. Cotton and Mr. Baker, who attended him, asked him if he believed in Christ, and felt that he was a sinner? He replied “I pray, but cannot feel.” The Sacrament of the Lord’s Supper was not administered to him, probably on account of his occasional delirium, and the generally disordered state of his mental faculties. At five minutes before eight yesterday morning he was pinioned by the executioner in the press room, in the presence of the sheriffs and officers of the goal. As St. Sepulchre’s church clock struck eight, the culprit, carrying the rope, attended by the executioner, and clergyman, moved in procession with the sheriffs, &c. on to the scaffold. On arriving at the third station, the prison bell tolled, and Dr. Cotton commenced at the same moment reading the funeral service “I am the resurrection and the life,” &c. of which the wretched man seemed to be totally regardless. On his being assisted up the steps of the scaffold, reason returned; he became aware of the dreadful death to which he was about to be consigned; his looks of terror were frightful; his expression of horror, when the rope was being placed round his neck, made every spectator shudder. It was one of the most trying scenes to the clergymen they ever witnessed – never appeared a man so unprepared, so unresigned to his fate. – The signal being given the drop fell, and the criminal expired in less than a minute. He never struggled after he fell. The body hung an hour, and was then cut down for interment. – The six unhappy men who are doomed to suffer on to-morrow morning, appear to be perfectly resigned to their fate. (Morning Chronicle)
CITATION: If you cite this Web page, please use the following citation: Rictor Norton (Ed.), “Newspaper Reports, 1823”, Homosexuality in Nineteenth-Century England: A Sourcebook, 29 December 2014; expanded 19 August 2016 http://rictornorton.co.uk/eighteen/1823news.htm
The case of Captain Rigby has everything a gay historian requires: sex, dramatic incident, humour, some degree of gay pride or at least defiance, personal human interest, and wider social relevance. It also holds together as an accessible story that can be easily grasped without the need for historical filters. The gay past here does not seem to be a different country, but a country very recognizeable to us today. Nevertheless, there is some historical context that would be useful to make some things more easily appreciated, which I mention in the following notes.
The following is the complete text of the trial of Captain Edward Rigby for sodomy in 1698. It documents the first recorded use of an agent provocateur, employed for the purposes of entrapment by the Societies for the Reformation for Manners. These Societies were formed in Tower Hamlets, London, in 1690, with their primary object being the suppression of bawdy houses and profanity. A network of moral guardians was set up, with four stewards in each ward of the City of London, two for each parish, and a committee, whose business it was to gather the names and addresses of offenders against morality, and to keep minutes of their misdeeds. By 1699 there were nine such societies, and by 1701 there were nearly 20 in London, plus others in the provinces, all corresponding with one another and gathering information and arranging for prosecutions.
Their first queer victim was Captain Edward Rigby. Early in 1698 he had been tried for sodomy at a court-martial, at which he was acquitted. But Reverend Thomas Bray, a leading member of the Societies for Reformation of Manners, believed Rigby to be guilty, and he worked out a plan with the constabulary to entrap him using as bait the servant named Minton who had previously been approached by Rigby. Minton’s master was Rev. Charles Coates, who was a parishoner of Thomas Bray. The trial below gives all the details.
Rigby’s trial was mentioned in several satirical ballads, including The Women’s Complaint to Venus.
The Societies for the Reformation of Manners were also responsible for the arrest of a group of sodomites in 1707, of whom several committed suicide while in prison. See The Tryal and Conviction of Several Reputed Sodomites.
Rigby’s trial is remarkable for showing that as early as the 1690s some men were aware of being part of a historical tradition: Rigby tells Minton, “it’s no more than was done in our Fore-fathers time.” As with many modern gay men, Rigby justified himself — and perhaps developed some sense of gay identity — by referring to historical figures and great men who were also gay.
It should be noted that his reference to Peter the Great is probably based upon first-hand evidence (I don’t think any biographer of Peter has referred to this contemporary evidence). Rigby must have observed Peter lying with Prince Alexander (a handsome lad Peter had picked up in the Moscow slums who became the most powerful man in Russia) during Peter’s visit to England from 11 January through 21 April 1698, aboard the royal yacht, or perhaps during Peter’s two-month stay in Deptford to examine the shipyards, where he caroused with the English sailors, or perhaps in the course of the sham naval battle that was staged for Peter’s entertainment on a visit to Portsmouth. Captain Rigby might well have had some official role to play during this state visit of the Russian monarch whose obsession was the buildilng of ships. Rigby had been made captain of the Mermaid fireship in 1693, and from 1695 until his arrest he commanded the Dragon, a 40 gun man- of-war in the squadron under Commodore Moody; he had taken two valuable prizes in the Mediterranean, and was an officer of some small fame.
Another man was indicted for aiding, abetting, and assisting Rigby in his sodomitical attempts, but was not named at the trial. He was probably Edward FitzGerald, one of two men with the same name, both of whom accused William Tipping, a clergyman, of suborning them to falsely charge Rigby with sodomizing them. Tipping was indicted for this conspiracy in July 1699, but the FitzGeralds’ charge was not believed, and the Grand Jury threw out the bill, with directions to seek out the two FitzGeralds to try them for perjury. Tipping was almost certainly another member of the Societies for the Reformation of Manners and a friend of Thomas Bray.
After serving his prison sentence, Rigby fled to France, where he became a Roman Catholic and entered the enemy’s service. In 1711 the French man-of-war the Toulouse was sighted by two English ships that were returning to Port Mahon in the Mediterranean. They engaged and captured her, and towed the badly damaged ship into port. The Second Captain of the Toulouse turned out to be none other than Edward Rigby. At Port Mahon the resourceful Captain Rigby found means to get on board a Genoese ship lying at anchor in the harbour, and by that means he again escape to France. He was highly regarded in France for his marine skills, and very well paid, though his pleasures were said to have been expensive.
The trial is preceded by several newspaper reports.
News Paper Reports
24 November 1698
There are now above 400 Prisoners in Newgate, 78 of whom are to Plead his Majesties Pardon next Sessions, and the rest are to come upon their Tryals, some of whom are for Buggery. (Dawks’s News-Letter)
10 December 1698
The Sessions is not yet ended, but 2 persons are convicted for that wicked crime of Buggery. (Dawks’s News-Letter)
Sat-Tues 10-13 December 1698
Yesterday the Trials ended at the Old Bailly [sic] when about 22 Criminals received Sentence of Death for different Crimes; a great many were Burnt in the Hand, and a certain Captain was fined in 1000 l. and ordered to stand 3 times in the Pillory for Buggery; as were some others for Misdemeanors, &c. Some others are Continued in Prison for Exchequer Notes, High-ways, &c. And then the Court Adjourned to 8 of the Clock on Friday Morning next, when above 70 persons are to plead their Pardons. Four Women that were Condemned to Die, pleaded their Bellies; and the Jury of Matrons returned 3 of them quick with Child, but the 4th otherwise. (The Flying Post)
13 December 1698
Yesterday the Tryials ended at the Old Bayly, when about 22 Criminals, received Sentence of Death for different Crimes, near 40 were Burnt in the Hand, and a Captain was Fined 1000l. and ordered to Stand 3 times in the Pillory for Buggery, and some others for other Crimes, &c. (Dawks’s News-letter)
17-20 December 1698
We are informed that a Man Servant, belonging to the Right Honorable the Lady Mary Howard, getting out of Bed on Monday morning last, came down Stairs, and putting himself in Womens Apparel, went up again to his Bed, and laid himself athwart it, and cut his own Throat. (The Flying Post) (Nearly the same report appeared in Dawks’s News-letter for 20 December.)
Tues-Turs 20-22 December 1698
On Tuesday last Captain Rigby stood in the Pillory, over-against the George Tavern in the Pall-Mall, and yesterday in Charing-Cross, according to Sentence, for attempting Sodomy; he appeared very gay. He is to stand again to morrow without Temple-Bar. (The Flying Post)
Tues-Thurs 20-22 December 1698
On Tuesday last Capt. Rigby stood upon the Pillory in the Pall Mall, before the George Tavern, and yesterday he stood at Chairing [sic Cross. (The Post Boy)
22 December 1698
Yesterday Captain Rigby stood on the Pillory at Charing Cross, and this day without Temple Bar. (Dawks’s News-letter)
Thurs-Sat 22-24 December 1698
On Thursday last Captain Rigby stood on the Pillory without Temple Bar, as did likewise two other Fellows in the Pillory within the Bar. (The Post Boy)
14 January 1699
I am informed that three other Indictments for Beastly Crimes are ready to be exhibited agianst Captain Rigby. (Dawks’s News-letter)
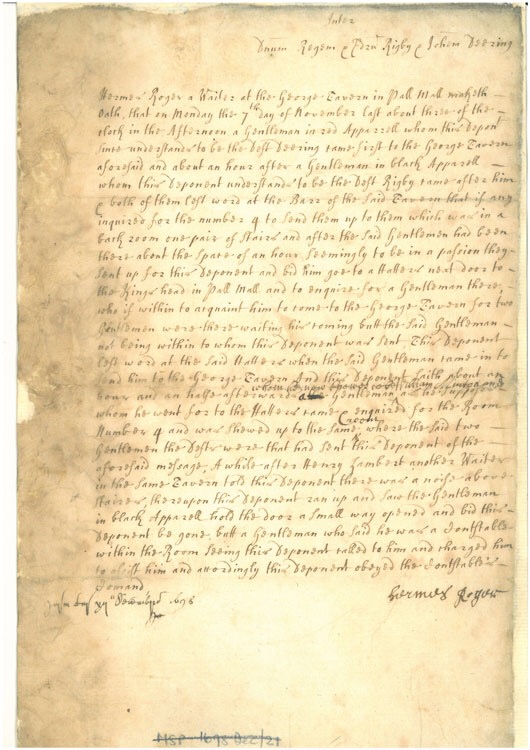
The Proceedings Against Captain Rigby
At the Sessions of Goal Delivery, held at Justice-Hall in the Old-Bailey, on Wednesday the Seventh Day of December, 1698. for intending to Commit the Abominable SIN of SODOMY, on the Body of one William Minton.
Printed by Order of the Court.
An Indictment was found against Captain Rigby, for that he, the Seventh day of November last, did Solicite, Incite, and as well by words as otherways, endeavour to perswade one William Minton (of about the Age of Nineteen Years) to suffer him the said Rigby, to commit the Crime of Sodomy with him the said Minton. And the said Rigby did also Endeavour and Attempt, to Commit the Crime of Sodomy with him the said Minton; and did also do and perpetrate divers other Enormities and abominable things, with an intent to Commit the Crime of Sodomy with the said Minton.
Captain Rigby being sensible of his Guilt, and unwilling the same should be disclosed to the World, would not therefore Plead Not Guilty to his Inditment; neither would he confess the same, but Demurr’d to the Indictment, in hopes, as his council alledged, that they might find some Fault therein; but upon Arguing the Demurrer, the Court were of Opinion the Indictment was good, and therefore Judgment was given against Rigby, which was the same as if he had Pleaded Guilty. And on the last day of the Sessions, the council for the King demanded Judgment against him, which could not be Adequate to his Crime; and for the Information of the Court, in order to give a Just and Exemplary Judgment, pray’d, That several Affidavits which were produced might be Read, which accordingly were Read; whereby it appeared,
That on Saturday the Fifth of November last, Minton standing in St. James’s Park, to see the Fireworks [i.e. the Guy Fawkes bonfire], Rigby stood by him and took him by the hand, and squeez’d it; put his Privy Member Erected into Minton’s Hand; kist him, and put his Tongue into Minton’s Mouth, who being much astonish’d at these Actions went from him; but Rigby pursued him, and accosted him again; and after much Discourse prevailed with Minton to tell him where he lodged, and to meet him the Monday following about Five a Clock, at the George- Tavern in the Pall mall, and to Enquire for Number 4. Minton the next day Acqainted Charles Coates, Esq; (with whom he lived) with what had happened to him the Night before, and desired his Advice and Direction therein; who with a Worthy Divine then present (being willing to detect and punish the Villany designed by Rigby) directed Minton to apply himself to Thomas Railto Esq; a Justice of the Peace for Middlesex; who being informed of what past between Rigby and Minton, appointed his Clark with a Constable, and two other Persons, to go with Minton to the George-Tavern, who were to stay in some Room adjoyning to the Room whereinto Minton should go: and if any Violence should be offered to him, upon crying out “Westminster” the Constable and his Assistance should immediately enter the Room.
That on Monday the Seventh of November last, about Four of the Clock in the Afternon, Rigby came to the George-Tavern, and left Number 4 at the Bar, with Directions, That if any Enquired for that Number, to send them to him; after Rigby had been about an Hour at the Tavern, (Minton not coming) Rigby called up one of the Drawers, and in a Passionte manner, bid him go to Minton’s Lodgings, and enquire for a young Gentleman; and if he were within, to tell him a Gentleman staid for him at the George-Tavern; the Drawer accordingly went, but Minton not being within, the Drawer return’d that Answer to Rigby.
That about six a clock Minton came to the George Tavern, enquired for Number 4. and was shewed into the room where Rigby was, and [t]he Constable and his assistance were placed in a Room adjoyning; Rigby seemed much pleased upon Mintons coming, and drank to him in a glass of Wine and kist him, took him by the Hand, put his Tongue into Mintons Mouth, and thrust Mintons hand into his (Rigby) Breeches, saying, “He had raised his Lust to the highest degree,” Minton thereupon askt, “How can it be, a Woman was only fit for that,” Rigby answered, “Dam’em, they are all Poxt, I’ll have nothing to do with them.” Then Rigby sitting on Mintons Lap, kist him several times, putting his Tongue into his mouth, askt him, “if he should F[uck] him,” “how can that be” askt Minton, “I’le show you” answered Rigby, “for it’s no more than was done in our Fore-fathers time”; and then to incite Minton thereto, further spake most Blaphemous words, and said, “That the French King did it, and the Czar of Muscovy made Alexander, a Carpenter, a Prince for that purpose,” and affirmed, “He had seen the Czar of Muscovy through a hole at Sea, lye with Prince Alexander.” Then Rigby kist Minton several times, putting his Tongue in his Mouth, and taking Minton in his Arms, wisht he might lye with him all night, and that his Lust was provoked to that degree, he had — [i.e. ejaculated] in his Breeches, but notwithstanding he could F[uck] him; Minton thereupon said, “sure you cannot do it here,” “yes,” answered Rigby, “I can,” and took Minton to a corner of the Room, and put his Hands into Mintons Breeches, desiring him to pull them down, who answered “he would not, but he (Rigby) might do what he pleased”; thereupon Rigby pulled down Mintons Breeches, turn’d away his shirt, put his Finger to Mintons Fundament, and applyed his Body close to Mintons, who feeling something warm touch his Skin, put his hand behind him, and took hold of Rigbys Privy Member, and said to Rigby “I have now discovered your base Inclinations, I will expose you to the World, to put a stop to these Crimes”; and thereupon Minton went towards the door, Rigby stopt him, and drew his Sword, upon which Minton gave a stamp with his foot, and cry’d out “Westminster”; then the Constable and his Assistance came into the Room, and seized Rigby, who offer’d the Constable a Gratuity to let him go, which he refusing, carryed Rigby before Sir Henry Dutton Colt, before whom Minton charged Rigby (who was present) with the Fact to the effect before related; who being askt by Sir Henry Colt, “Whether the Fact Minton had charged him with were True,” Rigby denyed not that the Charge against him was true, only objected against some inconsiderable Circumstances, which no ways tended to the lessening of the Charge.
That after all the Informations were read, Rigby was askt by the Court, “What he had to say for himself,” he desired that a Gentlemans Affidavit who was present when this matter was transacted might be read; the Court told him, “That that Gentleman stood Indicted in the same Indictment with him for being Aiding, Advising, and Assisting to him, in committing his Crime, and therefore could not be an Evidence for him.” Rigby was askt by the Court “what further he had to say,” he insisted on his Innocency, that he was misadvised by his Council in Demurring to the Inditment, which if he had known had been Confessing of the Fact in case the Court had been of Opinion that the Indictment was sufficient, he would not have done it; but seeing the Law was so he must submit to it; he said he was Drunk and might kiss Minton several times. To which it was answered by the Kings Council, “That his (Rigbys) Council had well advised him, and he knew his Guilt to be such, That it would be proved by Three or Four Witnesses beyond all contradiction,” and therefore Rigby Demurred to the Indictment, in hopes thereby his Crime would not be Disclosed, as it must have been if he had pleaded Not Gulty to his Indictment, and submitted to a Tryal; but as the Fact had now been made publick in Court; and it also appearing that he was not Drunk when he Committed it.
It was therefore prayed by the King’s Council, that the Court would give an Exemplary Judgment against him, for that Crime of which, by his own Confession, he stood Convicted, and was not in its Nature to be Aggravated.
And the Judgment which was pronounced by the Court against Rigby, was, viz.
That he stand Three several Days in the Pillory, for the space of two Hours, from Eleven of the Clock to One, in each of those days.
The first day over-against the George-Tavern in the Pall-mall; the Second day at Charing-Cross, and the Third day at Temple-Bar.
That he pay a Fine of 1000l. to the King.
That he lye in Prison for a Year, after he shall have paid his Fine.
And that before he be discharged out of Prison, he shall find sufficient Sureties for his good Behaviour for Seven Years.
Account of the trial for sodomy of Captain Edward Rigby (LMA reference MJ/SP/1698/12/024)References
SOURCE: An Account of the Proceedings against Capt Edward Rigby, London: Printed by F. Collins in the Old Bailey, 1698.
CITATION: If you cite this Web page, please use the following citation: Rictor Norton. Ed. “The Trial of Capt. Edward Rigby, 1698.” Homosexuality in Eighteenth-Century England: A Sourcebook. Updated 11 July 2013; http://rictornorton.co.uk/eighteen/rigby.htm
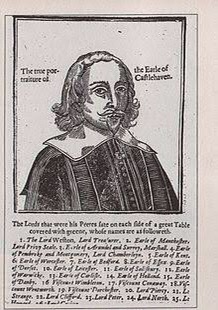
The 2nd Earl of Castlehaven, from a contemporary print published in the wake of his notorious trial.
Mervyn Tuchet (sometimes Mervin Touchet), 2nd Earl of Castlehaven (1593 – 14 May 1631), was an English nobleman who was convicted of rape and sodomy and subsequently executed.
A son of George Tuchet, 1st Earl of Castlehaven and 11th Baron Audley, by his wife, Lucy Mervyn, he was known by the courtesy title of Lord Audley during his father’s lifetime, so is sometimes referred to as Mervyn Audley.[1]
He was knighted by James I in 1608, before he studied law at the Middle Temple. He served as Member of the Parliament of England for Dorset in the Addled Parliament of 1614 and was a Justice of the Peace for the counties of Dorset, Somerset, and Wiltshire.[1] He succeeded his father on 20 February 1616/7 as Earl of Castlehaven and Baron Audley. He left seven children upon his death.[2]
Sometime before 1612 (records of the marriage are lacking), Lord Audley married Elizabeth Barnham, a sister-in-law of the philosopher and scientist Francis Bacon, and with her he had six children. By all accounts the marriage was a loving and successful one, ending with her death in 1622.[3] His second marriage, on 22 July 1624, at Harefield, Middlesex, was to the former Lady Anne Stanley (1580–1647), elder daughter and co-heiress of Ferdinando Stanley, 5th Earl of Derby (by his wife, Alice Spencer), and widow of Grey Brydges, 5th Baron Chandos. They had a daughter, Anne Touchet, who died young.[4] Lady Anne was significantly older than Castlehaven,[5] and the marriage was not a success, but in 1628 Lord Castlehaven’s son was married to her thirteen-year-old daughter, Elizabeth;[5] a marriage of step-children.
At a trial by his peers, it was stated that Henry Skipwith had arrived at Fonthill Gifford in 1621 and that within a few years he was so close to Castlehaven that he sat at the family’s table and was to be addressed as “Mister Skipwith” by the servants. Several years later, Giles Broadway arrived at the house and received similar treatment. It was not long before Castlehaven was providing Skipwith with an annual pension, and he was accused of attempting to have Skipwith inseminate his daughter-in-law, to produce an heir from Skipwith instead of his son. In fact, the countess and Skipwith had an adulterous relationship.
Castlehaven’s son, James, claimed that it was the extent of Castlehaven’s “uxoriousness” toward his male favourites which led to his initial lodging of a complaint in October 1630.[6]
Castlehaven’s trial aroused continuing public debate, and witnesses were almost certainly suborned. He maintained his innocence to the last, and the Privy Council was split on both charges, almost evenly on the sodomy charge. The case remains of interest to some as an early trial concerning male homosexuality, but ultimately its greatest influence proved to be as a precedent in spousal rights, as it became the leading case establishing an injured wife’s right to testify against her husband.[5]
Charges were brought against Castlehaven on the complaint of his eldest son and heir, who feared disinheritance, and were heard by the Privy Council under the direction of Thomas Coventry, Lord High Steward. Lady Castlehaven gave evidence of a household which she said was infested with debauchery, and the Attorney-General acting for the prosecution explained to the court that Castlehaven had become ill because “he believed not God”, an impiety which made Castlehaven unsafe. However, he insisted he was not guilty and that his wife and son had conspired together in an attempt to commit judicial murder. All witnesses against Castlehaven would gain materially by his death (as the defendant put it: “It is my estate, my Lords, that does accuse me this day, and nothing else”)[5] and “News writers throughout England and as far away as Massachusetts Bay speculated about the outcome.”[5]
Castlehaven was convicted, attainted, and three weeks later beheaded on Tower Hill for his sexual crimes: namely the “unnatural crime” of sodomy, committed with his page Laurence (or Florence) FitzPatrick, who confessed to the crime and was executed; and assisting Giles Browning alias Broadway, who was also executed, in the rape of his wife Anne, Countess of Castlehaven, in which Lord Castlehaven was found to have participated by restraining her.
The page who was executed, Laurence FitzPatrick, testified that Lady Castlehaven “was the wickedest woman in the world, and had more to answer for than any woman that lived”. In The Complete Peerage, Cokayne adds that the death of Castlehaven was certainly brought about by his wife’s manipulations and that her undoubted adultery with one Ampthill and with Henry Skipwith renders her motives suspicious. According to the historian Cynthia B. Herrup,[7] Anne was the equal of Lord Castlehaven in immorality.
Under the terms of the attainder, Castlehaven forfeited his English barony of Audley, created for heirs general, but retained his Irish earldom and barony since it was an entailed honour protected by the statute De Donis. When he was beheaded on Tower Hill on 14 May 1631, those Irish titles passed to his son James.
Mervyn Touchet’s first marriage (c.1611) was with Elizabeth Barnham (1592–c.1622/4), daughter of London alderman Benedict Barnham and his wife, Dorothea Smith, and they had six surviving children:
James Tuchet, 3rd Earl of Castlehaven (1612–1684), who married Elizabeth Brydges (1614/5–1679), daughter of his stepmother, but left no surviving children
Lady Frances Touchet (born 1617)
Hon. George Touchet (died c. 1689), who became a Benedictine monk
Mervyn Tuchet, 4th Earl of Castlehaven (died 1686)
Lady Lucy Touchet (died 1662)
Lady Dorothy Touchet (died 1635)
References
Ferris, John P.; Hunneyball, Paul (2010). “Audley, alias Tuchet, Sir Mervyn (c.1588-1631), of Stalbridge, Dorset; later of Fonthill Gifford, Wilts”. The History of Parliament.
Herrup 1999, p. ix.
Herrup 1999, p. 12.
[1]
a b c d e Herrup, Cynthia B. (January 2008) [2004]. “Touchet, Mervin, second earl of Castlehaven (1593–1631)”. Oxford Dictionary of National Biography (online ed.). Oxford University Press. doi:10.1093/ref:odnb/66794. (Subscription or UK public library membership required.)
Herrup 1999, p. 19.
Herrup, Cynthia B. (1999). A House in Gross Disorder: sex, law, and the 2nd Earl of Castlehaven. Oxford University Press.
Herrup, Cynthia (1999). A House in Gross Disorder: Sex, Law, and the 2nd Earl of Castlehaven. New York: Oxford University Press. ISBN 0-19-512518-5.
Lacey, Brian (2008). Terrible Queer Creatures: A History of Homosexuality in Ireland. Wordwell Books.
There is a plethora of information on the Vere Street Coterie, and it is a matter of sieving through it all to put this article on the event together. Considering the historic impact of the trial & punishment of members of the coterie, it is remiss that knowledge of it is not more widely spread. The 1810 conviction of London’s Vere Street Coterie led to the most brutal public punishment of homosexuals in British history.
The Vere Street Coterie began in 1810 when a man named Yardley introduced himself to James Cook. Yardley advised Cook that much money could be made by supplying the men of London with a male brothel. Cook, a self-proclaimed avaricious heterosexual, agreed to join Yardley in operating the White Swan in Vere Street, Clare Market.
The White Swan had a number of features designed to please its customers. The lower part of the house had one room with four beds, a ladies’ dressing room complete with every type of cosmetic, and a chapel for weddings.
Yardley and Cook followed the tradition established by the molly houses of the eighteenth century by allowing visitors to engage in sexual relations with each other free of charge. The upper section of the brothel housed prostitutes who lured casual customers in the manner of heterosexual brothels, presumably by wearing little clothing and offering various skills. No unusual interests, such as sadomasochism, were served.
The White Swan had been open for less than six months when the police raided it on July 8, 1810. Almost 30 of the inhabitants found themselves under arrest, including Cook. The police proved less of a problem than the mob, mostly female, who nearly killed the prisoners as they were transported in coaches from the watch house of St. Clement Danes to Bow Street for examination.
Most of the men were eventually set free for lack of sufficient evidence for prosecution. All seven of the men who were convicted belonged to the lower middle class, including William Amos, alias Sally Fox; Philip Kett; William Thomson; Richard Francis; James Done; and Robert Aspinal. Cook, found guilty of running a disorderly house, was never charged with sodomy.
All of the men except Aspinal were sentenced to stand an hour in the pillory. Aspinal had less culpability than the others and received a sentence of imprisonment for one year . Amos, for his third conviction on similar charges, received three years imprisonment, in addition to the pillorying. The others received terms of two years imprisonment, in addition to the pillorying.
The White Swan, The Gay Brothel in Vere Street – Lucy Inglis
Standing in the pillory involved locking the head and hands of a convict through one wing of a four-winged frame. The prisoner walked in a circle as the device rotated on an axis. The arrangement offered no means of protection to the convict.
On the day of the pillorying, September 27, 1810, the streets surrounding the Old Bailey were completely blocked by thousands of spectators. Shops were shut with the windows and roofs of nearby houses crowded with humanity. The mob, particularly the women, had built pyramids of mud balls that resembled shot. As the convicts moved in a wagon toward the pillory, the crowd hurled mud, dead cats and dogs, rotten fish, spoiled eggs, dung, offal, potatoes, turnips, brickbats, and verbal abuse. Several of the men began to bleed profusely from wounds.
Once placed in the pillory, the men walked for one hour while the violence continued unabated. About fifty women were permitted by authorities to form a ring among the men and pelt them incessantly. Cook and Amos, placed on the pillory without the protection of two additional prisoners’ bodies, suffered the worst, with Cook beaten almost insensible.
T wo members of the coterie, who were not present during the raid of July 8 but who were implicated by the testimony of an informer , were charged with buggery . Thomas White, a sixteen-year-old Drummer of the Guards in a Portugal regiment, and John Newbolt (or Newball) Hepburn, a forty-two-year-old ensign in a West India regiment, were captured after an acquaintance reported their involvement with the White Swan to a drum major . The officer arranged for both men to be brought for trial.
The Vere Street Gang at the pillory in 1810
Both soldiers were convicted and sentenced to death. They were hanged at Newgate prison on March 7, 1811.
The fate of the Vere Street Coterie terrorized the gay community in England. Part of a general crackdown on immoral behavior , the horrific punishment meted out to the group undoubtedly forced many gay men to re-evaluate their public activities.
Newspaper Reports of the Raid & Arrests
Tuesday, 10 July 1810
POLICE. Bow-Street, July 9. – In consequence of its having been represented to the Magistrates of the above office, that a number of persons of a most detestable description, met at the house of James Cooke, the White Swan, in Vere-street, Clare-market, particularly on a Sunday night, a privy search-warant was issued, and was put in execution on Sunday night last, when 23 persons, including the landlord of the house, were taken into custody, and lodged in St. Clement’s watch-house, till yesterday, at eleven o-clock,w hen they were brought before Mr. Read for examination; but the circumstance having transpired, a great concourse of people had collected in Bow-street, and which was much increased by the mob that followed the prisoners when they were brought from the watch-house. It was with the greatest difficulty the officers could bring them to and from the Brown Bear to the Office; the mob, particularly the women, expressing their detestation of the offence of which the prisoners were charged.
The following persons were first put to the bar, and gave their names and description:-
Esau Haycock keeps a shop near the Yorkshire Stingo, New Road.
James Amos, alias Fox, lodger, at the White Swan, (the house in question) a servant out of place, disabled in the arm. N.B. He was convicted and pilloried some time since for unnatural practices.
William Thopson, waiter at a hotel in Covent-garden.
Henry Toogood, servant to a gentleman in Portland-place.
Robert Aspinall, lodger, at No. 1, Brewer’s Court, Great Wild-street, taylor.
Richard Francis, a corporal in the 3d Regiment of Foot Guards.
James Cook, landlord of the house, and Philip Hot, the waiter.
Samuel Taunton, the officer, who had the executio of the warrant stated, that he and other officers went last night to the house about eleven o’clock, and apprehended the before-named persons, except the landlord and waiter, in a back parlour.
Two of the Patrole gave an account of their being in the house last night previous to the execution of the warrant [i.e. as infiltrators in disguise], and stated the particulars of the conversation and actions that passed while they were in the parlour, but it is of too horrible a nature to meet the public eye.
These witnesses also stated their having seen similar proceedings in the same parlour on the night of Sunday week, and identified several of the Prisoners as having been present at that time.
They were ordered to find bail for the misdemeanour, and in default were committed to prison.
James Spittle, a servant, in Chancery-lane; Matthew Saunders, of Duke-street, Aldgate; James Done, of Curran-road, shoreditch, bricklayer; William Barrow, of Furnival’s-inn; John Reeves, of Castle-street, Leicester-fields, traveller with goods, James Griffiths, Union-court, Holborn, servant out of place (well known at Bow-street); Edward Quaiffe, a soldier in the 3d Guards; George Boat, a waiter, out of place, lodging at the White Swan; John Clarke, Union-court, Holborn, a servant out of place; Timothy Norris, of Temple-street, Whitefriars, a servant out of place; Bernard Hovel, a soldier in the 1st Guards; Thos. Dixon, a soldier in the 3d Guards; Michael Hays, a servant out of place.
All these prisoners, except Dixon and Hays, who were in a dark kitchen, were found in a room on the first floor, but there being no evidence of what took place, they were all discharged except Done, who was proved to have been in the back parlour with the others, on the night of Sunday se’nnight. He was committed.
The crowd had, by this time, become so great in Bow-street, particularly facing the Office, that it was almost impossible to pass, and most of those who were discharged, were very roughly handled; several of them were hunted about the neighbourhood, and with great difficulty excaped with their lives, although every exertion was used by the constables and patrole to prevent such dangerous proceedings; and, in doing which, many of them were very roughly treated.
(Morning Chronicle; this newspaper cutting was pasted in William Beckford’s scrapbook now held in the Beinicke Library.)
Tuesday 10 July 1810
POLICE.
BOW-STREET, July 9.
On Sunday night, in consequence of some private information received by the Bow-street Magistrates, a strong party of police officers repaired to a public-house, the sign of the Swan, in Vere-street, Clare-market, said to be the rendezvous of a society of miscreants of a detestable description. The officers proceeded to search the house, where they found a company of 21 persons, the whole of whom, together with the landlord of the house, they apprehended, and lodged for the night in the watch-house of St. Clement’s parish. The house was a place of call for coffee-house and tavern waiters, and most of the persons taken were of that description. There were also amongst them some private soldiers of the Guards.
Yesterday morning, at eleven, the Bow-street officers proceeded with three coaches to the watch-house to bring up the prisoners for examination; but the concourse of people was so great that the carriages could scarcely proceed. Bow-street, and all the avenues leading to it, were also immensely crowded, and so continued till past 5 in the afternoon.
The prisoners underwent a long examination. Several were discharged, the proofs against them not being sufficiently strong to warrant their detention for trial; but their liberation was instantaneously productive of the most dangerous consequences. The multitude, male and female, fell upon them as they came out. They were knocked down, kicked, and covered with mud through every street in their endeavours to escape. The women, particularly those of Russel-street and Covent-garden market, were most ferocious in the application of this discipline; but the lower order of the male spectators were by no means lax in their exertions to mark their detestations of these wretches.
Out of the whole number, eight were ordered to find bail for the misdemeanour, and in default were committed to prison. They were housed for a time at the Brown Bear, in Bow-street, until the crowd should disperse. The crowd, however, continued to block up the Street and its avenues. A coach was drawn up before the door of the Brown Bear, for the conveyance of a part of the Delinquents to prison. This afforded a fresh signal to whet the eagerness of the mob, who pressed close round the carrige, and could not be kept off by the constables. It was, therefore, seen that any attempt to convey the Prisoners that way, must have exposed them to extremely rough handling, if not to urder. It was in consequence deemed prudent to detain the coach there, and by that means to fix the attention of the multitude, while the Prisoners were taken, about half-past four, over a wall at the rear of the Brown Bear, and into a large yard behind, which has an avenue to Russell-street, through which, after some time, they were conducted, hand-cuffed three together, to coaches, and conveyed to prison.
Tuesday 10 July 1810
POLICE.
BOW-STREET, July 9.
On Sunday night, in consequence of some private information received by the Bow-street Magistrates, a strong party of police officers repaired to a public-house, the sign of the Swan, in Vere-street, Clare-market, said to be the rendezvous of a society of miscreants of a detestable description. The officers proceeded to search the house, where they found a company of 21 persons, the whole of whom, together with the landlord of the house, they apprehended, and lodged for the night in the watch-house of St. Clement’s parish. The house was a place of call for coffee-house and tavern waiters, and most of the persons taken were of that description. There were also amongst them some private soldiers of the Guards.
Yesterday morning, at eleven, the Bow-street officers proceeded with three coaches to the watch-house to bring up the prisoners for examination; but the concourse of people was so great that the carriages could scarcely proceed. Bow-street, and all the avenues leading to it, were also immensely crowded, and so continued till past 5 in the afternoon.
The prisoners underwent a long examination. Several were discharged, the proofs against them not being sufficiently strong to warrant their detention for trial; but their liberation was instantaneously productive of the most dangerous consequences. The multitude, male and female, fell upon them as they came out. They were knocked down, kicked, and covered with mud through every street in their endeavours to escape. The women, particularly those of Russel-street and Covent-garden market, were most ferocious in the application of this discipline; but the lower order of the male spectators were by no means lax in their exertions to mark their detestations of these wretches.
Out of the whole number, eight were ordered to find bail for the misdemeanour, and in default were committed to prison. They were housed for a time at the Brown Bear, in Bow-street, until the crowd should disperse. The crowd, however, continued to block up the Street and its avenues. A coach was drawn up before the door of the Brown Bear One of those committed is a soldier; the reset of them flashy dressed fellows, in coloured clothes, with nankeen trowsers, silk stockings, &c. all hale robust fellows, the oldest not above 33.
Tuesday 10 July 1810
POLICE.
BOW-STREET, July 9.
On Sunday night, in consequence of some private information received by the Bow-street Magistrates, a strong party of police officers repaired to a public-house, the sign of the Swan, in Vere-street, Clare-market, said to be the rendezvous of a society of miscreants of a detestable description. The officers proceeded to search the house, where they found a company of 21 persons, the whole of whom, together with the landlord of the house, they apprehended, and lodged for the night in the watch-house of St. Clement’s parish. The house was a place of call for coffee-house and tavern waiters, and most of the persons taken were of that description. There were also amongst them some private soldiers of the Guards.
Yesterday morning, at eleven, the Bow-street officers proceeded with three coaches to the watch-house to bring up the prisoners for examination; but the concourse of people was so great that the carriages could scarcely proceed. Bow-street, and all the avenues leading to it, were also immensely crowded, and so continued till past 5 in the afternoon.
The prisoners underwent a long examination. Several were discharged, the proofs against them not being sufficiently strong to warrant their detention for trial; but their liberation was instantaneously productive of the most dangerous consequences. The multitude, male and female, fell upon them as they came out. They were knocked down, kicked, and covered with mud through every street in their endeavours to escape. The women, particularly those of Russel-street and Covent-garden market, were most ferocious in the application of this discipline; but the lower order of the male spectators were by no means lax in their exertions to mark their detestations of these wretches.
Out of the whole number, eight were ordered to find bail for the misdemeanour, and in default were committed to prison. They were housed for a time at the Brown Bear, in Bow-street, until the crowd should disperse. The crowd, however, continued to block up the Street and its avenues. A coach was drawn up before the door of the Brown Bear The crowd was not dispersed from Bow-street and its vicinity till near six o-clock, and appeared to be extremely mortified at the escape of their intended victims. (The Times, Issue 8029)
Thursday 12 July 1810
[ADVERTISEMENT]
ON Monday, the 9th day of July, 19810, as one of the Prisoners, that was taken up for an unnatural crime, was gong up Tavistock-street, Covent-Garden, after being acquitted by the Sitting Magistrate ofBow street Police Office, THOMAS HAYLETT, a young Man in the employ of a respectable Tradesman, in Tavistock-street, did assault and beat the above-mentioned acquitted person; and upon Mr. Rt. Shearsmith, Watch-maker, of No. 41, Stanhope-street, Clare market, from motives of humanity, requesting the said Thomas Haylett to desist from beating the man, he (T. H.) branded Mr. Shearsmith with being one of the disgraceful party, and did without any other provocation, strike Mr. Shearsmith a violent blow on the mouth, by which blow he nearly lost two or three teeth; for which unwarrantable attack the said Thomas Haylett doth thus publicly ask pardon of Mr. Shearsmith, in consideration of which, and the good character he bears, Mr. S. has condescended not to prosecute him.
&nsp; &nsp; &nsp; &nsp; THOMAS HAYLETT.
Witness – M. K. SUPPLE.
Morning Advertiser)
Monday, 16 July 1810
POLICE. DIABOLICAL CLUB IN VERE-STREET.
Bow-Street. – On Friday evening Esay Haycock, who was apprehended with a number of other persons at the White Swan public-house, in Vere-street, Clare-market, where they met, it was supposed, for the purpose of committing a most detestable offence, was brought to the Office from New Prison, Clerkenwell, and was admitted to bail himself in 100l. and James Smith, of Buckingham-street, New Road, in 50l. and John Colley, of York-street, Blackfriars-road, to 50l. for the prisoner to answer for the offence with which he is charged at the Sessions.
Henry Toogood, another of the persons who was apprehended at the same house with the same persons, was also brought from the prison, and was admitted to bail in 100>l. and two sureties, Wm. Baker, of Silver-street, Clerkenwell-green, and Wm. Wye, of Bunhill-row, in 50l. each.
Application was made on Saturday night to bail Cook, the landlord of the public house, but it was put off till this day.
(Morning Chronicle. From this report we can see how risky it was for any friends to provide sureties for a suspected sodomite, for their names would be published in the newspapers. Incidentally, according to the Morning Chronicle for 17 July 1810, Mr Nares the Magistrate refused Cook’s application for bail. Also incidentally, the Morning Chronicle for Thursday, 26 July 1810, reported the suicide “yesterday morning” of Mr Tranter, a footman in the service of the Prince of Wales, in Carlton House.)
17 July 1810
LONDON SESSIONS, MONDAY, JULY 16.
JOHN BARLOWE and WOLFE LYON, the latter a Jew, about 60 years of age, were indicted as accomplices in a high misdemeanour, with intent to commit a detestable crime, on the night of the 24th of April last. The Prosecutor, Scranton, having cause to suspect the intention of the Traversers, watched them from George-street, behind the Mansion-house, to a dark alley leading from Bearbinder-lane, into Lombard-street, where he detected them in the fact; he secured on the spot. But Lyon made his escape; and the Prosecutor apprehended him some weeks afterwards, in St. Paul’s Church-yard. The Prisoners were both found guilty. Lyon had been already twice convicted of the like offence. The first time in 1796, for which he was imprisoned in Newgate three years, and held in recognizance, hiimself in 100l. and two sureties for 50l. each, for three eyears after the expiration of his sentence; and the second time in 1805, when he was sentenced to four years imprisonment and similar recognizances. The Court, in consideration of his being thus shewn to be an incorrigible offender, ordered his second recognizance to be estreated [i.e. forfeited], and himself to be iimprisoned five years in Newgate: and to find the like recognizance for seven years after the expiration of his sentence.
Barlowe, who is a young man, and had been a Gentleman’s servant, was sentenced to two years imprisonment, and the same recognizances as Lyon.
THOMAS SINEY was indicted for an assault with the like intent upon a youth, named Nicholson, in Moorfields, on the 29th April. The assault was clearly proved. The prisoner, in a sanctified tone, made a long speech in his defence. – said he was coming from a place of worship, and that it was the prosecutor who made the assault upon him. He said he had been but three weeks in London, and was going from the Tabernacle to his lodgings in Tash-street, Gray’s-inn-lane, but he produced no witnesses even to character.
Verdict Guilty.
the Court sentenced him to two years imprisonment, and the like recognizance as in the preceding cases. (The Times, Issue 8036)
18 July 1810
At the Clerkenwell Sessions yesterday, four persons, of the names of Ramsey, Clarke, Goff, and Hill, were found guilty of an attempt to extort 10l. from T. Fitzhugh, a gentleman’s servant, by threatening to charge him with an unnatural offence.
Friday, 27 July 1810
Yesterday at Bow-street, the Ensign brought up by Revett, the officer, from the Isle of Wight, in consequence of a charge agaisnt him of an inhuman offence, at the Swan public house in Vere-street, underwent an examination before Mr. Justice Birnie. It is horrible to hear of the multiplied instances of this detestable crime; and in none have the circumstances been more atrocious, or the charge more distinctly proved. We, of course, abstain from all detail. The prisoner’s name is Hepburn, an Ensign belonging to a West India Regiment. He was fully committed to Newgate to take his trial, on the oath of a drummer in the Guards. (Morning Chronicle, Issue 12859)
Wednesday 1 August 1810
Yesterday at Bow-street, the Ensign brought up by Rivett, the officer, from the Isle of Wight, in consequence of a charge against him of a detestable offence, at the Swan public-house, in Vere-street, underwent an examination before Mr. Justice Birnie. It is horrible to hear of the multiplied instances of this detestable crime; and in none have the circumstances been more atrocious or the charge more distinctly proved. We, of course, abstain from alldetail. The prisoner’s name is Hepburn an Ensign belonging to a West India regiment. He was fullyi committed in Newgate to take his trial, on the oath of a drummer in the Guards. (Hereford Journal)
Saturday, 4 August 1810
Wednesday Dickinson, who was convicted at the last Westminster Sessions, of an assault upon a drum boy in the Guards, was exhibited, for an hour, on the pillory, at Charing-Cross; and received a most pitiless pelting from the indignant multitude, with mud, eggs, turnips, and other missiles. He is a well looking young man, about 22, and was a waiter at Hatchett’s hotel, Piccadilly. In the course of the first 10 minutes he was so completely enveloped with mud and filth, that it was scarcely possible to distinguish his back from his front; and it was with the utmost difficulty that the peace officers could prevent him from being torn to pieces by the mob, on his return from the pillory to the prison. (Ipswich Journal, Issue 4013)
Saturday, 18 August 1810
CHELMSFORD, August 17.
At our Assizes, . . . Samuel Mounser was convicted of an unnatural crime, and received sentence of death. (The Ipswich Journal, Issue 4015)
20 September 1810
OLD BAILEY, WEDNESDAY, SEPT. 19.
John Newbold Hepburn, aged 42, Ensign in a West India regiment, and Thomas White, a drummer in the guards, aged 16, were put to the bar on a capital indictment for a most detestable crime. but on the application of Hapburn founded on his affidavit that two drummers, now with their regiments in Portugal, were material witnesses for his defence, the trial was postponed until next session. (The Times)
Saturday, 29 September 1810
MIDDLESEX SESSIONS, SEPTEMBER 22.
Seven of the detestable club of Vere-street, viz. Wm. Amos, alias Fox, James Cooke, Philip Ilett, Wm. Thompson, Richard Francis, James Done, and Robert Aspinal, were tried for conspiring together at the Swan, in Vere-street, Clare-market, for the purpose or exciting each others to commit a detestible offence. Mr. Pooley stated the case for the prosecution, and the witnesses against the prisoner were Nichols, and another of the Bow-street patrole, who were sent to the house by the Magistrates, to watch the proceedings of persons assembled there. They gained admittance into the back parlour, which was the principal rendezvous of these miscreants, and were considered as persons of the same propensity, and treated without reserve. For three nights they witnessed such disgusting conduct and language, as to place beyond all doubt the intentions of the company. They gave information of all they had seen, and the prisoners, with a number of others, were brought before the Magistrates. The evidence being closed, Mr. Gurney, who had cross-examined the witnesses while giving their testimony, said that he was placed in the aukward [sic] situation of Counsel for the defendants, and had undertaken that task because he felt himself bound to do so by his oath, and duty as an advocate. In the course of the evidence he had done that duty to the best of his judgment, by giving the defendants every benefit of cross-examination. But he found the testimony so clear and uncontradicted, as to leave no ground of palliation upon which to make any appeal to the Jury, upon circumstances, which, if true, would go to excite an idea that the horrors of Sodom and Gomorrah were revied in London. He must therefore decline trespassing on the time of the Jury, and leave them to form their own conclusions. If the prisoners had any thing to offer in their defence, he had no doubt they would meet with every indulgence. The prisoners being then called on, each told his story, but it could have made no impression on the minds of any discerning Jury, and all the prisoners were found Guilty. Amost, having been trice before convicted of similar offences, was sentenced to three years imprisonment, and to stand once in the pillory in the Hay-market. Cooke, the keeper of the house, Ilett, Thompson, Francis, and Done, were sentenced to two years imprisonment, and the pillory in the same place; and Aspinal, to one year’s imprisonment only.
On sentence being pronounced they were all handcuffed, and tied to one chain in Court, and ordered to Cold Bath-fields prison. On leaving the Court, a numerous crowd of people, which had collected at the door, assailed them with fists, sticks, adn stones, which the constables could not completely prevent, although they were about 40 in number. The prisoners perceiving their perilous situation, immediately ran in a body to the prison, which they reached in a few minutes, and the constables, by blockading the streets, prevented the most fleet of their assailants from molesting them during their inglorioius retreat. (Jackson’s Oxford Journal, Issue 2996)
26 September 1810
An exhibition on the pillory of one of the wretches recently convicted at Clerkenwell took place yesterday, at 12 o’clock, opposite the Mansion-house when this human monster suffered all that could be inflicted by mud, rotten eggs, and potatoes.
The concourse of people collected upon this occasion was immense. Amongst other places particularly crowded was the ballustrade surrounding the Mansion-house, which, notwithstanding the exertions of constables placed there to keep off the crowd, was filled with spectators, some of whom had melancholy reason to regret their too eager curiosity as several of the rails and a great part of the coping stone gave way from the great weight of those clinging to it, and falling on some of the persons beneath, severely injured three, one of whom is not expected to recover; they were all taken to the Hospital. (The Times, Issue 8098)
Saturday, 29 September 1810
MIDDLESEX SESSIONS. — Unnatural Crimes. Seven of the infamous club of Vere-street, viz. Wm. Amos, alias Fox, James Cooke, Philip Islet, William Thompson, Richard Francis, James Done, and Robert Aspinal, were tried on Saturday, and all found Guilty.
Amos having been twice before convicted of similar offences and punished, was sentenced to three years imprisonment, and to stand once in the pillory, in the Hay-market, opposite Panton-street.
Cooke, the keeper of the house, Ilett, thompson, Francis and Done, were each sentenced to two year’s imprisonment, and the pillory in the same place; and Aspinal, as not having appeared so active as the others, to one year’s imprisonment only.
Four other wretches of the same description were found Guilty. (Leeds Mercury, Issue 2358)
27 September 1810
Notices were yesterday issued by the Sheriffs of Middlesex to all their officers, to appear this morning with their javelins at Newgate, for the purpose of escorting the Vere-street squad to the Haymarket, where they are to exhibit their faces precisely at 12 o’clock. (The Times)
Friday, 28 September 1810
PILLORY. – Yesterday William Amos, alias Fox, James Cook (the landlord), Philip Bell (the waiter), William Thomson, Richard Francis, and James Done, six of the Vere-street gang, stood in the Pillory, in the centre of the Hay-market, opposite Norris-street. They were conveyed from Newgate in the open caravan used for the purpose of taking the transports [i.e. those sentenced to transportation] to Portsmouth, in which they were no sooner placed, than the mob began to salute them with mud, rotten eggs, and filth, with which they continued to pelt them along Ludgate-hill, Fleet-street, the Strand, and Charing-cross. When they arrived at the Hay-market, it was found that the pillory would only accommodate four at once. At one o’clock, therefore, four of them were placed on the platform, and the two others were in the meantime taken to St. Martin’s Watch-house. The concours of people assembled were immense, even the tops of the houses in the Hay-market were covered with spectators. As soon as a convenient ring was formed [i.e. a space around the pillory], a number of women were admitted within side, who vigorously expressed their abhorrence of the miscreants, by a perpetual shower of mud, egs, offal, and every kind of filth with which they had plentifully supplied themselves in baskets and buckets. When the criminals had stood their allotted time, they were conveyed to Coldbath-fields Prison. At two o’clock the remaining two were placed in the Pillory, and were pelted till it was scarcely possible to adistinguish the human shape. The caravan conveyed the two last through the Strand, then to Newgate, the mob continuing to pelt them all the way. Notwithstanding the immense concourse of people, we are happy to learn that no accident occurred.
The horrible exhibition of yesterday must prove to every considerate spectator the necessity for an immediate alteration in the law as to the punishment of this crime. It is obvious that mere exposure in the pillory is insufficient; – to beings so degraded the pillory of itself would be trifling; it is the popular indignation alone which they dread: and yet it is horrible to accustome the people to take the vengeance of justice into their own hands. We avoid entering into the discussion of a crime so horrible to the nature of Englishmen, the prevalence of which we fear we must ascribe, among other calamities, to the unnecessary war in which we have been so long involved [i.e. the Napoleonic Wars]. It is not merely the favour which has been shown to foreigners, to foreign servants, to foreign troops, but the sending our own troops to associate with foreigners, that may truly be regarded as the source of the evil. For years we have observed with sorrow the progressive reovlution in our manners; and we have uniformly and steadily opposed all the innovations that have been admired in our theatres and our select places of amusement, as destructive of their character of the country.
Many of the most illustrious persons who at first charged us with illiberality, are now convinced of the right view which we took of the subject, and are zealously disposed to exert themselves in stemming a torrent of corruption that threatens to involve us in the gulph of infamy as well as ruin. We trust that the very first object of Parliament, on its meeting, will be the revision of this law.
(Morning Chronical. This newspaper cutting was pasted into William Beckford’s scrapbook, now at the Beinicke Library)
28 September 1810
Yesterday [i.e. 27 Sept.], Cooke, the Publican of the Swan in Vere-street, Clare-market, and five others of the eleven miscreants convicted at Clerkenwell Sessions last Saturday, of detestable practices, were exhibitedin the Pillory in the Hay market, opposite to Panton-street. Such was the degree of popular indignation excited against these wretches, and such the general eagerness to witness their punishment, that, by ten in the morning, the chief avenues from Clerkenwell Prison and Newgate to the place of punishment were crowded with people; and the multitude assembled in the Haymarket, and all its immediate vicinity, was so great as to render the streets impassible. All the windows and eventhe very roofs of the houses were crowded with persons of both sexes; and every coach, waggon, hay-cart, dray, and other vehicles which blocked up great part of the street, were crowded with spectators.
The Sheriffs, attended by two City Marshals, with an immense number of constables, accompanied the procession of the Prisoners from Newgate, whence they set out in the transport caravan, and proceeded through Fleet-street and the Strand; and the Prisoners were hooted and pelted the whole way by the populace. At one o- clock four of the culprits were fixed in the pillory, erected for and accommodated to the occasion, with two additional wings, one being alloted for each criminal; and immediately a new torret of popular vengeance poured upon them from all sides. The day being fine, the streets were dry and free from mud, but the dfect was speedily and amply supplied by the butchers of St. James’s- market. Numerous escorts of whom constantly supplied the party of attack, chiefly consisting of women, with tubs of blood, garbage, and ordure from their slaughter-houses, adn with this ammunition, plentifully diversified with dead cats, turnips, potatoes, addled eggs, and other missiles, the criminals were incessantly pelted to the last moment. They walked perpetually round during their hour [the pillory swivelled on a fixed axis]; and although from the four wings of the machine they had some shelter, they were completely encrusted with filth.
Two wings of the Pillory were then taken off to place Cooke and Amos in the two remaining ones, and although they came in only for the second course, they had no reason to complain of short allowance, for they received even a more severe discipline than their predecessors. On their being taken down adn replaced in the caravan, they lay flat in the vehicle; but the vengeance of the crowd still pursued them back to Newgate, and the caravan was so filled with mud and ordure as completely to cover them.
No interference from the Sheriffs and Police officers could refrain the popular rage; but notwithstanding the immensity of the multitude, no accident of any note occurred. (The Times, issue 8100; Most of this report was reprinted verbatim in the Annual Register, vol. 52, Chronicle entry for 27 September 1810)
28 September 1810
The disgust felt by all ranks in Society at the detestable conduct of these wretches occasioned many thousands to become spectators of their punishment. At an early hour the Old Bailey was completely blockaded, and the increase of the mob about 12 o’clock, put a stop to the business of the sessions. The shops from Ludgate Hill to the Haymarket were shut up, and the streets lined with people, waiting to see the offenders pass. Four of the latter had been removed from the House of Correction to Newgate on Wednesday evening, and being joined by Cook and Amos, they were ready to proceed to the place of punishment.
A number of fishwomen attended with stinking flounders and entrails of other fish which had been in preparation for several days.
The gates of the Old Bailey were shut and all strangers turned out. The miscreants were then brought out, all placed in the caravan. Amos began to laugh, which induced his companions to reprove him, and they all sat upright, apparently in a composed state, but having cast their eyes upwards, the sight of the spectators on the tops of the houses operated strongly on their fears, and they soon appeared to feel terror and dismay.
At the instant the church clock went half-past twelve, the gates were thrown open. The mob at the same time attempted to force their wayin, but they were repulsed. A grand sortie of the police was then made. About 60 officers, armed and mounted as before described, went forward with the City Marshals. The caravan went next, followed by about 40 officers and the Sherriffs. The first salute received by the offenders was a volley of mud, and a serenade of hisses, hooting, and execration, which compelled them to fall flat on their faces in the caravan. The mob, and particularly the women, had piled up balls of mud to afford the objects of their indignation a warm reception.
At one o’clock four of them were exalted on a new pillory, made purposely for their accommodation. The remaining two, Cook and Amos, were honoured by being allowed to enjoy a triumph in the pillory alone.
Upwards of fifty women were permitted to stand in the ring [in front of the pillory], who assailed them incessantly with mud, dead cats, rotten eggs, potatoes, and buckets filled with blood, offal, and dung, which were brought by a number of butchers’ men from St James’s Market. These criminals were very roughly handled; but as there were four of them, they did not suffer so much as a less number might.
After an hour, the remaining two, Cook and Amos, alias Fox, were desired to mount and in one minute they appeared a complete heap of mud and their faces were much more battered than those of the former four.
Cook appeared almost insensible, and it was necessary to help him both down and into the cart, whence they were conveyed to Newgate by the same road they had come. As they passed the end of Catherine Street, Strand, on their return, a coachman stood upon his box, and gave Cook five or six cuts with his whip.
From the moment the cart was in motion, the fury of the mob began to display itself in showers of mud and filth of every kind. Before the cart reached Temple Barm, the wretches were so thickly covered with filth, that a vestige of the human figure was scarcely discernible. They were chained, and placed in such a manner that they could not lie down in the cart, and could only hide and shelter their heads from the storm by stooping. This, however, could afford but little protection. Some of them were cut in the head with brick-bats, and bled profusely. The streets, as they passed, resounded with the universal shouts and execrations of the populace. (The Times)
Note: For a long report about this incident in the pillory, see Newspaper Reports for 3 October 1810.
29 September 1810
The Bow-Street officers and patrol apprehended many pickpockets in the crowd during the pilloring of Cook et al., including Samuel Brooke; William Hall; John Fregeur, a porter at the Saracen’s Head, Snow Hill; George Cohen. (The Times)
29 September 1810
We understand that in consequence of a proposition from Cooke the Publican, and one of the miscreants who were pilloried in the Hay-market on Thursday, there was a meeting of the Westminster Magistrates on Wednesday evening, to consider his offer for discovering a number of his accomplices in the same abominable system, but in a very different rank in life, provided his punishment of the Pillory was remitted; but that the Magistrates, after full deliberation, deemed it more for the advantage of public morals to reject his proposition, and let the sentence of the law take its course. (The Times, Issue 8101)
Monday, 1 October 1810
LONDON,
THURSDAY, SEPTEMBER 27, 1810
PILLORY. — Six of the monsters of the Vere-street Club were exhibited in the Pillory, in the Hay-Market, on Thursday. Between 30 and 40,000 persons were present. The indignation of the populace was so great that they scarcely escaped with their lives. (Hampshire Telegraph and Sussex Chronicle, Issue 573)
Tuesday, 2 October 1
James M’Namara, a low vulgar Irishman, seemingly a bricklayer’s labourer, and Thomas Walker, a squalid looking lad of about 17, a soldier in the first regiment of Guards, were tried for a similar crime, on the 14th ult.; and George Horiby, a cobbler, and John Cutmore, a soldier, were indicted for a similar crime, at the Star and Crown public-house, in Broadway, Westminster, on the 21st July. All four were found guilty. – Sentence deferred. (The Hull Packet and Original Weekly Commercial, Literary and General Advertiser, Issue 1238; the full report of the trial was otherwise identical with that reported by Jackson’s Oxford Journal for 29 September. The same brief report appeared in the Morning Chronicle for 24 September, which added the sentence “All four were caught in the fact.”)
Wednesday, 7 November 1810
MIDDLESEX SESSIONS, Nov. 6.
—— Haycock and —— Cooley, two of those miscreants who were apprehended at the Swan, in Vere-street, in July last, were convicted and sentenced to be imprisoned in the House of Correction for two years. (Morning Chronicle, Issue 12947)
6 December 1810
OLD BAILEY.
Yesterday the Sessions commenced before the RECORDER of LONDON, Mr. NATHANIEL GROSE, and Baron GRAHAM.
John Newbold Hepburn, formerly an officer in a West India regiment, and thomas White, late a drummer in the guards, (whose trials had been put off at the last and preceding sessions), were capitally indicted for perpetrating with each other a detestable crime, at Vere-street, Clare-market,, upon tesmony of another drummer in the guards, named R. MANN, and both found guilty. Hepburn is aged 42; White only 18. (The Times, Issue 8159)
Thursday, 6 December 1810
OLD BAILEY
These Sessions commenced yesterday before Mr. Justice Grose, Mr. Baron Graham, the Lord Mayor, Recorder, and Common Serjeant.
Thomas White and John Newball Hepburn stood capitally indicted for having committed an unnatural offence on the 17th of May last.
It was formerly mentioned, that the two delinquents were apprehended, shortly after the discovery of the detestable society in Vere-street, upon the accusation of a drummer, named James Mann, belonging to the 3d Regiment of Guards.
It appeared, from the testimony of Mann, that the Prisoner Hepburn accosted him on the Parade in St. James’s Park, a few days before the day on which the offence charged was committed: he told him that he was very anxious to speak to the boy who was then beating the big drum, meaning White, and said he would reward him if he would bring the lad to his lodgings, at No. 5, St. Martin’s Church-yard. Mann said he would tell White what he had said, and they then parted, Hepburn presenting him with half-a-crown. In the evening Mann and White went to Hepburn’s lodgings, who received them with great cordiality, and informed them that he belonged to a veteran regiment and was shortly going to the Isle of Wight. – Mann then went on to state that Hepburn invited them to dine with him on the ensuing Sunday at his lodgings, but to this White objected, observing it was not a good place, and proposed at the same time that they should meet at the Swan, in Vere-street. To this Hepburn agreed, and an appointment was accordingly made, which was punctually observed by all parties. On their arrival at the Swan, on Sunday, they were shewn into a private room where they had dinner; before and after which, conduct the most vile and disgusting passed between the two prisoners, the particulars of which it is impossible to detail without a gross violation of decency. It was on the detection of the monsters in Vere-street that Mann communicated the facts already stated to his Drum Major [presumably Mann had been linked to those arrested at the White Swan, and had agreed to testify against White and Hepburn to save his own skin], in consequence of which information White was instantly confined, and an officer was sent to the Isle of Man for Ensign Hepburn, the particulars of whose apprehension have already been stated.
The charge was most clearly and indisputably proved, and the Prisoners were both found Guilty – DEATH.
(Morning Chronicle. This newspaper cutting was pasted into William Beckford’s scrapbook, now at the Beinecke Library)
Monday, 10 December 1810
On Wednesday Ensign John Newbolt Hepburn, of the 4th West India Regiment (whose apprehension at the Barracks at Newport was stated in a former paper) and T. White, a drum boy, were tried at the Old Bailey, for a detestable crime. The prisoner Hepburn accosted Mann, the boy, whose evidence supported the prosecution, while on parade in the Park, promising to introduce him to White. The witness and White afterwards received an invitation to dine with him, and they met at the house in Vere-street, where the detestable gang was discovered some time since, and dragged to punishment. In consequence of information communicated by Mann to the Serjeant-Major of his Regiment, the prisoners were apprehended. Hepburn called several persons to speak to his character, but they did not attend. One witness, however, (Colonel Grant) stated that the prisoner had served in the same Regiment with him in 1794, and during that time Colonel G. had not heard any complaint against him. The other prisoner, White, also called a witness, who gave him a good character for orderly behaviour in his Regiment. The Jury found both prisoners – Guilty. the prisoner Hepburn is 42 years of age. (Hampshire Telegraph and Sussex Chronicle, Portsmouth, Issue 583)
The following description of the White Swan was written by the lawyer Robert Holloway, in his remarkable but trustworthy account The Phoenix of Sodom, or The Vere Street Coterie (London, 1813):
The fatal house in question was furnished in a style most appropriate for the purposes it was intended. Four beds were provided in one room – another was fitted up for the ladies’ dressing-room, with a toilette, and every appendage of rouge, &c. &c. A third room was called the Chapel, where marriages took place, sometimes between a “female grenadier”, six feet high and a “petit maitre” not more than half the altitude of his beloved wife! There marriages were solemnized with all the mockery of “bridesmaids” and “bridesmen”; the nuptials were frequently consummated by two, three or four couples, in the same room, and in the sight of each other. The uper part of the house was appropriated to youths who were constantly in waiting for casual customers; who practised all the allurements that are found in a brothel, by the more natural description of prostitutes. Men of rank, and respectable situations in life, might be seen wallowing either in or on beds with wretches of the lowest description.
It seems the greater part of these quickly assumed feigned names, though not very appropriate to their calling in life: for instance, Kitty Cambric is a Coal Merchant; Miss Selina a Runner at a Police Office; Blackeyed Leonora, a Drummer; Pretty Harriet, a Butcher; Lady Godiva, a Waiter; the Duchess of Gloucester, a gentleman’s servant; Duchess of Devonshire, a Blacksmith; and Miss Sweet Lips, a Country Grocer. It is a generally received opinion, and a very natural one, that the prevalency of this passion has for its object effeminate delicate beings only: but this seems to be, by Cook’s account, a mistaken notion; and the reverse is so palpable in many isntances, that Fanny Murry, Lucy Cooper, and Kitty Fisher, are now personified by an athletic bargeman, an Herculean Coal-heaver, and a deaf Tyre-Smith: the latter of these monsters has two sons, both very handsome young men, whom he boasts are full as depraved as himself. These are merely part of the common stock belonging to the house; but the visitors were more numerous and, if possible, more infamous, because more exalted in life: and “these ladies”, like the ladies of the petticoat order, have their favorite men; one of whom was White a drummer of the guards, who, some short time since, was executed for sodomy with one Hebden, an ensign.
White, being an universal favourite, was very deep in the secrets of the fashionable part of the coterie; of which he had made a most ample confession in writing, immediately previous to his execution; the truth of which he averred, even to his last moments.
That the reader may form some idea of the incontrollable rage of this dreadful passion, Cook states that a person in a respectable house in the city, frequently came to his pub, and stayed several days and nights together; during which time he generally amused himself with eight, ten, and sometimes a dozen different boys and men!
Sunday was the general, and grand day of rendezvous; and to render their excuse the more entangled and doubtful, some of the parties came a great distance, even so much as thirty miles, to join the festivity and elegant amusements of grenadiers, footmen, waiters, drummers.
Friday, 1 March 181THE PRINCE REGENT’S COURT.
Yesterday, at one o’clock, his Royal Highness the Prince Regent held a Court and Privy Council at Carlton House. Soon after one his Royal Highness gave audiences to the Lord Chancellor, Earl Camden (the Lord President of the Council), Sir Joseph Banks, and Mr. Pinkney, the american Minister. . . . His Royal Highness afterwards held another Council, which, in addition to the above, was attended by Lord Ellenborough, for receiving the Recorder of London’s report of the capital convicts at the December and January Old Bailey Sessions (except those for forgery), including Ensign Hepburn, and White the drummer, for an abominable offence, who were ordered for execution next Thursday; the others were respited during his Royal Highness’s pleasure. (Morning Chronicle, Issue 13045)
Friday, 8 March 1811
EXECUTION. — Yesterday morning, about five minutes efore 8 o’clock, Ensign Hepburn, and —— White, the drummer, a lad, only 16 years of age, for the perpetration of an unnatural crime, were brought on the scaffold, in front of the Debtors’ door, Newgate, and executed pursuant to their sentence. Their conduct since condemnation has been such as to evince a sincere contrition, and a just sense of the heinousness of their offence. They behaved in a manner becoming their unhappy situation; and after spending a few minutes in fervent prayer and devotion, with the Rev. Dr. Ford the Ordinary of Newgate, were launched into eternity, amidst a vast concourse of spectators. (Morning Chronicle, Issue 13051)
Saturday, 9 March 1811
The Duke of Cumberland, Lord Sefton, Lord Yarmouth, and several other Noblemen, were in the Press Yard, when Hepburn and his associate were executed. (Morning Chronicle, Issue 13052)
Monday, 11 March 1811
EXECUTION. — On Thursday, J. N. Hepburn, late an Ensign in a Veteran Battalion, and Thomas White, late a drum-boy in the Guards, were executed in the Old Bailey, pursuant to their sentence in December Sessions, for a crime of the most revolting nature. — Hepburn was 42 years of age, and White 17. White came out first; he seemed perfectly indifferent at his awful fate, and continued adjusting the frill of his shirt while he was viewing the surrounding popoulace. About two minutes after Hepburn made his appearance, but was immediately surrounded by the Clergyman, Jack Ketch [i.e. the hangman], his man, and others in attendance. The Executioner at the same time put the cap over Hepburn’s face, which of course prevented the people from having a view of him. White seemed to fix his eyes repeatedly on Hepburn. After a few minutes prayer, the miserable wretches were launched into eternity. Hepburn spoke to the Shieriff in a very firm and impressive manner, stating that the person who had sworn against him had perjured himself, and that every inta [? piece of evidence?] that he (Hepburn) had said, to prove the perjury, was perfectly correct. The Duke of Cumberland, Lord Sefton, Lord Yarmouth, and several other Noblemen, were in the Press Yard. (Hampshire Telegraph and Sussex Chronicle, Portsmouth, Issue 596)
Wednesday, 13 March 1811
EXCESSIVE GRIEF. — The mother of White, the Drummer, who was executed on Thursday, with Hepburn, the Ensign, died of a broken heart on the day subsequent to her son’s untimely end. She never left her bed after having taken farewell of the culprit on the evening previous to his execution. (Morning Chronicle, Issue 13055)
1811 – Thomas White & John Newbolt Hepburn of the Vere Street Coterie
Two centuries ago today, two men were hanged at Newgate Prison for buggery as a result of one of 19th century England’s most notorious anti-gay police raids.
Brits whose sexual palate ran beyond the stiff upper lip braved the force of the law to frequent molly houses, private clubs catering to homosexuality, cross-dressing, and the like.
In 1810, bobbies* busted mollies at one such establishment at the White Swan in London’s Vere Street. A press which evidently preferred its nicknames as vanilla as its coition dubbed these apprehended sodomites the Vere Street Coterie.
According to Phoenix of Sodom, a lasciviously queer-loathing account of the Coterie’s misadventures and of “the vast geography of this moral blasting evil” infesting London,
The fatal house in question was furnished in a style most appropriate for the purposes it was intended. Four beds were provided in one room – another was fitted up for the ladies’ dressing-room, with a toilette, and every appendage of rouge, &c. &c. A third room was called the Chapel, where marriages took place, sometimes between a “female grenadier”, six feet high and a “petit maitre” not more than half the altitude of his beloved wife! There marriages were solemnized with all the mockery of “bridesmaids” and “bridesmen”; the nuptials were frequently consummated by two, three or four couples, in the same room, and in the sight of each other. The upper part of the house was appropriated to youths who were constantly in waiting for casual customers; who practised all the allurements that are found in a brothel, by the more natural description of prostitutes. Men of rank, and respectable situations in life, might be seen wallowing either in or on beds with wretches of the lowest description.
It seems the greater part of these quickly assumed feigned names, though not very appropriate to their calling in life: for instance, Kitty Cambric is a Coal Merchant; Miss Selina a Runner at a Police Office; Blackeyed Leonora, a Drummer; Pretty Harriet, a Butcher; Lady Godiva, a Waiter; the Duchess of Gloucester, a gentleman’s servant; Duchess of Devonshire, a Blacksmith; and Miss Sweet Lips, a Country Grocer. It is a generally received opinion, and a very natural one, that the prevalency of this passion has for its object effeminate delicate beings only: but this seems to be, by Cook’s account, a mistaken notion; and the reverse is so palpable in many instances, that Fanny Murry, Lucy Cooper, and Kitty Fisher, are now personified by an athletic bargeman, an Herculean Coal-heaver, and a deaf Tyre-Smith: the latter of these monsters has two sons, both very handsome young men, whom he boasts are full as depraved as himself. These are merely part of the common stock belonging to the house; but the visitors were more numerous and, if possible, more infamous, because more exalted in life.
This intriguing little window into proto- or pre-gay culture opens to us at some cost to its participants, six of whom were confined to the pillory where the mob (“chiefly consisting of women”) bombarded them
with tubs of blood, garbage, and ordure from their slaughter-houses, and with this ammunition, plentifully diversified with dead cats, turnips, potatoes, addled eggs, and other missiles … They walked perpetually round during their hour [the pillory swivelled on a fixed axis]; and although from the four wings of the machine they had some shelter, they were completely encrusted with filth … On their being taken down and replaced in the caravan, they lay flat in the vehicle; but the vengeance of the crowd still pursued them back to Newgate, and the caravan was so filled with mud and ordure as completely to cover them.
Worse was to come.
Not arrested on the initial bust or included on the pillory, a 16-year-old regimental drummer named Thomas White was snitched out by a fellow-drummer for having also been a White Swan regular … and in fact, “an universal favourite … very deep in the secrets of the fashionable part of the coterie.”
The stool pigeon’s motivation was the usual in such cases: said pigeon was also making a bit on the side from the Coterie, and he had a mind to avoid his own self being completely covered with mud and ordure and dead cats and turnips.
This James Mann’s report to his superior officer, and subsequent testimony to the magistrates, got White and his partner in vice Ensign John Hewbolt Hepburn hanged for sodomy.
Our correspondent in Phoenix of Sodom notes the presence among that “vast concourse of people” who witnessed their deaths several nobles whom he clearly takes to be a vanguard of that homosexual agenda, “the Duke of Cumberland, Lord Sefton, Lord Yarmouth, and several other noblemen.” No word on Miss Sweet Lips or Blackeyed Leonora.
Merrie Olde England would go on issuing hempen discharges to gay soldiers for years to come.
As a footnote, the Rev. John Church, who might be the earliest openly homosexual Christian minister in England, was rumored to have performed gay marriages at the club.
CITATION: If you cite this Web page, please use the following citation:
Rictor Norton (Ed.), “The Vere Street Club, 1810”, Homosexuality in Nineteenth-Century England: A Sourcebook, 7 May 2008, updated 7 September 2008 http://rictornorton.co.uk/eighteen/1810vere.htm
Originally written in 2001. This article has never been published.
I have come to realise, perhaps a bit late in life, that you spend far too much time bending in the general direction of things instead of sticking up for yourself and saying no, this is not what I want, or the way I want things to go!
I have decided to sue a local hospital. That I have chosen to do this has come as a tremendous shock to me, though those around me seem to have been waiting for me rectify what has been, for me, a life changing event.
By 1996 I had accepted that sooner or later, AIDS was going to get me. What I hadn’t counted on was that St. Vincent’s hospital was going to assist in my chances of survival! – and in the one ward they had where I always felt I would be safe – Ward 17, the dedicated HIV/AIDS ward.
It was a sudden change in health status that delivered me to the A&E department. I had collapsed outside my apartment building, gasping for breath, clutching my chest, thinking that a heart attack was going to beat AIDS to the crunch, or that PCP had finally caught up to me, as it seemed to do to all in my state. It turned out to be neither – I had a collapsed left lung, though being HIV, they moved me into Ward 17 after inserting a tube to keep the lung inflated. Most of us assume that we go into hospital to be cured of health problems, or at least receive a better standard of medical care to assist you to a slightly higher standard of health than you have when you enter. Well…I have to tell you it doesn’t always happen that way!
I firmly believe that some people go into health care because they truly believe in what they are doing. They truly believe they can make a difference, that they can benefit people who are ill or are disabled. These people are not professors of medicine, do not have a fancy examination room with a prestigious address, and are not heads of departments. The well-heeled medico’s who share these attribute have strings of initials after their names. They do ward rounds with a string of nose-in-the-air arse lickers and sycophants. St Vincent’s at this time had more than its fair share of the latter, and unfortunately, some of them were in HIV medicine!
Now, I don’t want to give the impression that I was just in hospital with a collapsed lung – it was more complicated than that. I was in the midst of changing doctors, so didn’t actually have a GP when I was admitted to Ward 17. My scripts for AZT had just run out, I had chronic anaemia, chronic Candida, and weighed in at about 48 kilos. In other words, I was a very sick boy. Now, under normal circumstances, with a CD4 count of about 10, they would test and examine you for ALL AIDS related illnesses – PCP, CMV, MAC, neurological and psychological problems. For some unknown reason. Sure, they treated – and eventually repaired – the collapsed lung. They tested me for PCP – negative result – and gave me a blood transfusion, but that was it. No eye examination, no dietician, no occupational therapist – no, that’s a lie, I did have one session with an OT, and though she promised other sessions – she never quite madeit back.
So I lay there for 10 days, drifting in and out of sleep, as you tend to do when you are in this bad a condition, suffering in silence the daily ward rounds with a professor who seemed more interested in prestige than care, with his little band of sycophants, who seemed to assume that this was what was expected of theM. No one seemed to particularly care, so I was thankful for friends, for without them I think I would have gone mad.
Death seemed pre-ordained at this time I felt I had outlived everyone else anyway, and that my time was drawing to a close. I had predicted 2 years when I quit work to go on the pension in 1993, and had managed 3, so in many respects I felt I had survived beyond expectation, and short of a miracle, I was going through the final stage of my life. I was, to all intended purposes, fulfilling expectation.
So, with a repaired lung, a couple of pints of fresh blood, and some Candida medication, I was discharged 10 days later. No HIV medications, no doctor. I had my discharge papers sent to a local HIV GP, who I didn’t know from a bar of soap, hoping that she would feel sorry for me, and rush me through the waiting list. Thankfully, she did just that!
Two days out of hospital, and her receptionist rang to say my discharge papers had arrived, and that even though they didn’y know who I was, the doctor wanted to see me. I would like to think, in hindsight, that this was almost like some sort of sign, as having my hospital discharge sent to her was an act of providence that probably saved my life.
As soon as I mentioned to her that my vision had been ‘greying over’ for a couple of weeks, she was immediately on the phone to the Prince of Wale’s Hospital Eye Clinic at Randwick. They promised that somebody would stay back at the end of clinic until I arrived to have my eyes checked. They thought at that stage that I had CMV retinitis, but could not be certain enough to confirm the diagnosis. I had to travel to Hurstville the next day to see a leading ophthalmologist, an expert in CMV. He confirmed the diagnosis, and by the time I arrived home that afternoon, their was a message to ring the doctor. She wanted me admitted to Prince Henry Hospital straight away.
Prince Henry added other health items to the list St Vincent’s had. On top of chronic anaemia and Candida, and my 10 CD4 cells, they added chronic bilateral CMV retinitis, and Wasting Syndrome. Pandemonium was about to strike, but at least this time I felt as though people cared. Prince Henry was much more grounded in reality than St Vincent’s, and whatever my prognosis may have been – mortality was never discussed – they went out of their way to help me. Sure, I had a drip in both arms, was being transported to Prince of Wales twice a week for intraocular injections of ganciclovir, and I was a bit of a guinea pig because of my condition – medical students must love people like me, as we become a living text book – but they did care. I had a dietician who planned meals and snacks for me, and nurses on hand to help me during my night sweats. I even had a reporter from Japan interview and photograph me, as he was doing a piece to be published in Japan. After seeing me, he was concerned that the Japanses ‘head-in-the-sand’ attitude to HIV/AIDS was something to be seriously concerned about.
To be honest, the two weeks in Prince Henry gave me a different perspective on many aspects of life. There was the guy in the room next to mine – I had a huge room to myself in Marks Pavilion, and the windows looked out over Beauty Bay – who had terminal cancer. Not once, despite whatever he may have been going through, did I hear him complain or whinge about his lot. He virtually lived in the hospital, and even had his own stereo moved in with him. And the young guy who was at the opposite end of the ward to me. He also had CMV, but fuck, he was so young, so innocent! We sat together in the eye clinic one day, and he grasp[ed my hand, cuddled up to me, and cried. I wanted to give him some hope, but I would have felt like such a hypocrite. I didn’t know if their was hope for me at that stage, let alone try to give it to someone else who I knew was worse off than I was.
Well, they saved my sight – sort of! The injections, and eventually $10,000 worth of ‘Vitrasert’ ganciclovir implants managed to save the sight in my left eye. As for my right eye, the optic nerve was damaged by the CMV, and despite efforts on everyones part, I lost 80% of the vision in it, and the impact on my life has been…disconcerting. I have regular checks every few months now, and I have to be careful not to bump my head hard on anything. The scar tissue in the left eye is so dense that they are concerned now about me ending up with a detached retina. I’ve also had two operations to remove cataracts caused by the implants. They originally estimated a 4% chance of cataracts from the implants, but 12 months later this prediction was upgraded to a 100% chance. Some odds you can’t beat.
But this has been the least of my worries. Sure, my right eye has, in some respects, compensated for the loss of vision in my left, but not entirely. It took me twelve months to adjust, but that twelve months was not without incidents, such as tripping over some tree roots in Crown Street, and landing flat on my face in front of some people coming in the opposite direction. I also tripped and stumbled a great deal as my vision tried to compensate for a change in everything, including perspective. Stairs with contrasting edging strips became ramps – at least from my perspective – and ‘I’m sorry!’ became part of my everyday vocabulary as I bumped and staggered my way around. That is something that even 5 years down the line, I have never quite gotten used to. This would not be the first time I have stated that in some respects, it would have been easier to have ended up completely blind. At least that way, I would have a white cane, or a dog, and people would know I was definitely blind, and not give me condescending looks every time I run into someone. For some unknown reason, it has always ended up my fault. I just accept.
Rules of our household – don’t leave anything sitting low on the floor, or hanging to my left when I don’t know it is there. When walking down the street, keep to my right. If you don’t keep to that side, expect me to keep moving to ensure you are there. Go into the city? Not on my own these days. As much as I love the city, and love to watch it grow, it is a place for people in a rush, not a place for people who are visually impaired. Too many people, too many doorways for them to rush out of, and too many people crushing into confined spaces. I miss it very much, but it is not a place for me anymore. I shop locally, and that is hazardous enough for me. Do anything during the peak hour rush? Not likely these days. I had to meet David at 6.00 at the Entertainment Centre, to attend a couple of concerts. I actually mapped out a way to get there that would have a minimum of people that I would have to avoid. I go to daytime lectures and tutorials at UTS to avoid travelling too and fro during peak hours. I’m also trying to get them to contrast edge-strip the black granite stairs in the Tower Building, so that visually impaired people can see where the stair edges are. That is one fight I may yet win. Oh, and I shouldn’t forget that I kick small children.
David, who is my partner, and I went for a walk down Hall Street, leading to Bondi Beach, for one reason or another – we were probably looking for somewhere to eat breakfast. Sure enough, for a split second, I wasn’t watching where I was going and the next thing I knew, this kid had run straight onto my foot as I took a step forward. He just came out of nowhere, as kids do, and I managed to literally lift him into the air with the forward motion of my step, and launched him off to the side of the footpath. Thankfully, he landed in the grassed area around some trees growing on the footpath. I would hate to think what may have happened if he had landed on the footpath itself. I don’t know who got the biggest fright – the kid, myself, the kid’s father, or David. The father came running as I picked the kid up to make sure he was okay, but the look on the father’s face said it all – It was my fault, and I should have been watching where I was going. Even an explanation that I was partially blind, and hadn’t seen the kid coming didn’t seem to sit well with him, nor did a multitude of apologies. Now, I dare say the kid probably forgot the incident 10 minutes after it happened, but It is still a nightmare with me. Whenever I think about the state of my eyes, that is the one instant that comes straight to mind. It’s not just the incident with the kid – I’m aware of that. It is that in some way, these sorts of things happen to me everyday, though fortunately with larger adults, not small kids. Despite all my precautions, despite taking my time getting around, despite walking metres up a street to use crossings or lights, despite great care at intersections I feel it is only a matter of time before I either seriously hurt somebody, or they seriously hurt me.
So I’m not just going to sit back and cop it sour anymore. Somewhere along the line, in a hospital, on a particular time on a particular day, somebody, for whatever reason, decided not to do something, and now I’m paying the price. Well, it’s time for someone to pay for their oversight, and the time to pay is NOW! My health is as good as it’s going to get at the moment, and with it being unlikely that I will ever return to full-time work, or to any job that requires me to get stressed, it is time to take action. I’m not going to ignore it anymore, or pretend that it just didn’t happen. It did, and my life has never been the same since.
Personally, I think that they, like Prince Henry, and certainly me, never expected me to live, so just doing a minimum of care in 1996 may have been acceptable practise, especially in an area of medicine that has always been cash strapped. But I didn’t die! I am well and truly alive, and the time for revenge is at hand. I hope that at the end of the day, they will learn several lessons. Never assume anything; never underestimate the strength of the human will, and mind; and never think people are just going to forget about it! We Don’t!
Tim Alderman
P.S: despite the solicitor instigating an action against St Vincent’s, and doing this pro-bono, I was expected to pay the bills for photocopying and incidentals. I received a bill for $1,500 from them to cover this…and being on a pension, this was the beginning, and the end, of the action. Justice never was served.
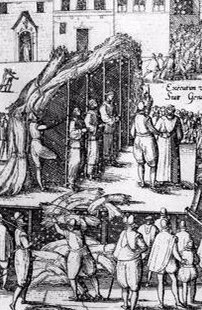
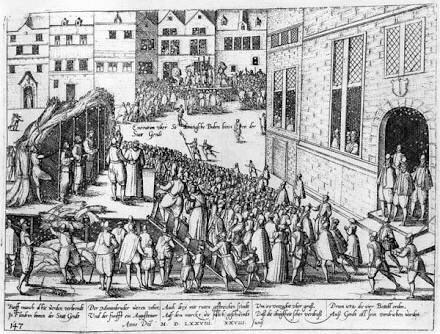 References
References